Problems in the sphere of healthcare of the Russian Federation. Modern high technologies. Problems of public administration in the field of health care and ways to solve them








Description of the presentation Social problems of health care. One of the main slides
One of the main tasks of state policy in Russia is to ensure the protection of life and health of the population, the solution of which could contribute to the sustainable socio-economic development of the country. Currently, there are many social risks in Russia that pose a threat to the life and health of the population. The side effects of socio-economic transformations, the depletion of natural resources as a result of irrational use solely for the purpose of making a profit against the background of an increase in the technical equipment of many state-important facilities, lead to the creation of an increasing threat not only to the life and health of the country's population, but to all of humanity. The powerful mutagenic effect of radioactive radiation, electromagnetic fields, X-ray and infrared radiation, and other harmful factors used in industry leads to the destruction of the country's gene pool and human degradation. Social risks for a person are also represented by the consequences of a spiritual and moral crisis. The lack of an ideology of creation among modern youth, their own destructive life activity, the lack of basic medical knowledge and skills, the ability to provide themselves with safe work and living conditions most often leads to catastrophic consequences. The structure of society, depopulation and degradation of the population, the growth of corruption and crime are of concern. Up to 0.5 million people predominantly males die in road accidents, on water bodies, in case of alcohol and drug poisoning, during "showdowns", suicide, law enforcement, while serving in the army. As a result, only 14 million men are able to start a family.
The most tangible loss of population occurs during road traffic accidents. According to the WHO, every year 10 million people die as a result of road traffic accidents in the world, and from 20 to 50 million people become disabled, which brings enormous social and economic damage to the entire human community. According to the World Bank, the global economic losses to humanity amount to about $ 500 billion a year. Due to the unfavorable environmental situation, the incidence rate among the population is steadily increasing (see Fig.). The highest incidence in Russia with a diagnosis established for the first time was registered in Karelia and Altai Territory (over 1000 cases per 1000 population), from 800 to 1000 population - in Arkhangelsk, Tver, Leningrad, Murmansk, Arkhangelsk, Orenburg, Tyumen, Irkutsk regions and in Yakutia. From 500 to 800 thousand cases per 1000 population were registered in Smolensk, Bryansk, Volgograd, Astrakhan, Saratov, Sverdlovsk, Chelyabinsk, Tomsk, Novosibirsk, Chita and Amur regions, Krasnoyarsk and Krasnodar regions, in Buryatia and Tyva. The lowest morbidity (up to 500 cases per 1000 population) is registered in the Khanty-Mansi Autonomous Okrug (Yugra), Yamalo-Nenets, Taimyr and Evenki Autonomous Okrugs.
Morbidity per 1000 population in the regions of Russia (registered patients with a diagnosis established for the first time in 2006) There is a clear increase in psychiatric pathology in Russia. Mental abnormalities are noted in 20% of the population. There is a sharp increase in the number of children born sick or sick during the neonatal period. During the period from 2000 to 2006, this figure reached 40% of the total number of children born alive. There are 14 million disabled people in Russia, including 523 thousand children. This indicates a low level of quality of medical care and social rehabilitation in the country. The effectiveness of rehabilitation of disabled people in our country is from 3 to 6.5%, and in the USA - from 15 to 20%. At the same time, the health care system, drug and medical services are not working efficiently enough. The main reason for the low efficiency of the population health protection system is the underfunding of this industry from the state. Thus, in the United States and other developed countries, financing the health care system is considered the task of the state and amounts to 15% or more of GDP. In Russia, the health care system is financed on a leftover basis, expenditure items are cut and mainly industrial and military-industrial sectors are supplied. At the same time, only 2.5 -3% of GDP is planned for health care, which is in no way compatible with the current demographic situation in the country. Funds directed by a targeted order are not always used for their intended purpose, as a result of which the population is forced to turn to private clinics, which most often cannot afford the majority of the population of Russia. In order to resolve this situation in 2007, 328.2 billion rubles were allocated for the implementation of the basic compulsory health insurance program. At the same time, the compulsory medical insurance system practically does not work. The very system of organizing medical assistance to the population suffers. Currently, medical care in Russia is provided at the following levels: polyclinic, ambulance and inpatient care. Outpatient and polyclinic care is provided in 9620 institutions, including 833 dental clinics. Given the vast territory of Russia, this number is negligible. Moreover, each polyclinic is staffed with local doctors and honey. sisters, on average, only 30%. Low salaries and a huge workload of doctors (up to 1,500-4,000 thousand people per district doctor) leads to a decrease in the efficiency of the treatment process and overload of polyclinics. The sanitary-educational and preventive work is not even mentioned. Dental care is now practically inaccessible to the population. The prices for dental care are unreasonably high and are 3-5 times higher than their cost. As a result, dental clinics are empty, as the population prefers not to go there for help and visits the dentist only in emergency cases.
Ambulance services are provided by about 3268 stations. They are insufficiently equipped with reanimation vehicles and medicines and are absolutely not protected from encroachments by criminal structures. As a result of the huge number of traffic jams on the road, the ambulance cannot get to the call at the right time, and the patient often dies, or his further treatment is complicated. About 1.8 million people die each year due to more than 24 hours delay in admission to the hospital. Ambulance teams are insufficiently staffed with qualified personnel, and there is no unified communication system between various ambulance stations. In this regard, it is necessary to ensure that 2-3 ambulances are on duty for each microdistrict, so that the speed of rendering honey. aid did not depend on the condition of roads and traffic jams. The system of protection of mothers and children suffers. Despite the widespread government programs that stimulate the birth rate, the perinatal service in Russia is currently ineffective. There is a low level of health of pregnant women, 80% of pregnant women have concomitant pathology: anemia, cardiovascular disease, kidney disease, edema and proteinuria, diabetes mellitus, etc. As a result, only 24.6% of births are proceeding normally. Basically, childbirth is pathological, as a result of which 30% of children are born sick or get sick in the first days of life. The system for the prevention of infectious diseases in children is also ineffective. At present, in Russia the so-called compulsory "vaccination calendar" includes 10-15 compulsory vaccinations. In European countries, the number of compulsory preventive vaccinations for children has reached 150 or more. The issue with the production of Russian baby food, dietary baby food for children with phenylketonuria and various types of fermentopathies has not been resolved, the range of baby food is extremely poor, and its production in Russia is not envisaged.
Thus, ensuring the protection of life and health of the population, the formation of a healthy lifestyle should be carried out in the following areas: · In the field of ensuring the safety of life and health of the population, it is necessary to continue developing a system for protecting and improving the environment; creation of ensuring access of the population to daily monitoring of the state of the environment. · In the field of ensuring health care and high quality medical services for the population, it is necessary to increase funding for health care, medical services and social services to 15% of GDP; develop strategies to improve the quality of health care services, reduce premature, especially preventable mortality, and reduce morbidity. · In the field of maternal and child health, due to the increase in the number of concomitant pathologies during pregnancy and childbirth, increase the period of prenatal maternity leave and arrange it from 16 weeks, placing a pregnant woman in a day hospital, creating an "incubator" for nursing pregnant women in order to prevent pathology in childbirth , mothers' schooling and treatment. In the field of the formation of the ideology of a healthy lifestyle among the population, it is advisable to obligatory introduction of health-saving pedagogical technologies and medical and hygienic disciplines in preschool, secondary and higher education institutions in order to foster a culture of health and a healthy lifestyle in children, adolescents and youth, the widespread introduction of anti-alcohol and anti-nicotine projects in schools, colleges and universities, at work, the fight against drugs and the introduction of a system of fines for drinking and smoking in public places; creation of motivation by employers for a healthy lifestyle.
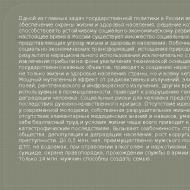
According to experts (Note 3), the main problems should be attributed (Figure 1):
- 1) Personnel problems in the health care system such as: lack of qualified personnel (13.0%), the presence of problems in personnel policy (salary level, working conditions) (11.0%) and low-quality and degrading training of modern personnel (10, 4%).
- 2) Reduced influence and control of modern politics (17.5%).
- 3) Deficit financing of the healthcare system (11.7%).
Figure 1 - Significant problems of the development of the health care system in the Russian Federation,%
Staffing of the health care system
The first important personnel problem is the lack of qualified personnel. As of January 1, 2015 in medical organizations of the system of the Ministry of Health of Russia in the constituent entities of the Russian Federation there are 580 431 doctors and 1 287 659 medical workers with secondary vocational education. The indicator of the ratio of the number of doctors and nurses in the Russian Federation in 2014 was 1 to 2.3, which corresponds to the value provided for by the state program. The provision of the population of the Russian Federation (per 10 thousand) with doctors is 40.3, paramedics - 100.0
According to the data of the Accounts Chamber, in Russia as a whole, 90 thousand workers in the medical sector were laid off. The largest reduction affected doctors of clinical specialties - more than 19 thousand people (excluding doctors working in medical organizations of the Crimean Federal District).
According to the audit of the Accounts Chamber, today there is a need for doctors and nurses in the amount of 55 thousand and 88 thousand people. Thus, the implemented measures to reduce the number of medical workers do not correspond to the actual situation in the regions and the current need. An analysis of the ongoing personnel measures is required, and, as a result, their possible adjustment.
The second important problem is the presence of problems in personnel policy (salary level, working conditions). In general, at the end of 2014, the wages of public sector employees in absolute terms increased. According to Rosstat data, the average salary of doctors in 2014 compared to 2013 increased by 4.0 thousand rubles, nursing (pharmaceutical) personnel - by 2.2 thousand rubles, junior medical personnel - by 1.8 thousand rubles.
However, the level of salaries of medical workers is greatly influenced by the high percentage of internal part-time jobs, which makes up a quarter of the total payroll. This means that the increase in the level of the average salary of medical workers is caused not by an actual increase in the size of their remuneration, but by an increase in the workload on one worker, when, instead of the prescribed 8 hours, the doctor works 12 hours or more.
The third important problem is poor quality and degrading training of personnel. The conducted expert survey showed that there is insufficient training of personnel, unsatisfactory qualifications of medical personnel and, as a result, low quality of medical care.
The fourth important problem is the outflow of professional staff to the private sector. Experts have noted a tendency for the outflow of professional personnel to the private sector. The population of Russia began to use paid services more and more, in 2014 there was an increase in the volume of paid medical services - by 24.2% compared to 2013. As the auditor of the Accounts Chamber notes, in the context of a decrease in the availability of medical care for the population, an increase in paid medical services services may indicate the replacement of free medical care with a paid one.
Health system financing
Based on data from the United Nations, World Health Organization and World Bank, Bloomberg Bloomberg Best (and Worst). Most Efficient Health Care 2014: Countries has presented a ranking of countries in the world in terms of health systems performance in 2014. Bloomberg's annual rating on the effectiveness of national health systems ranked Russia last - 51st (1st place - Singapore, Germany - 23rd place, Azerbaijan - 49th place). The criteria for assessing health care are: life expectancy, per capita health care costs, the ratio of health care costs to the state's GDP. Let's compare several countries - the leaders are Singapore, Italy, Germany, the USA and Russia (Table 1).
Table 1 - Indicators of the effectiveness of national health systems.

In the presented rating, undoubtedly, life expectancy is the dominant indicator of the effectiveness of the health care system in a particular country. According to the data, the table shows that today the Russian health care system in relation to developed countries can be conditionally called lagging and "catching up".
3. And also the expert community expressed the following problematic aspects in the health care system (Figure 4): low quality of services and drugs provided (8.1), commercialization of the medical industry, including corruption (5.8), inaccessibility of some services and drugs (5.2), the ambiguous attitude of people (patients) to modern medicine (lack of respect, culture) (5.2), low level of medical equipment. institutions with the necessary medicines and equipment (3.2), insufficient introduction of innovations and technologies (1.9), high dependence on foreign manufacturers and technologies (1.3), the influence of external independent factors (0.6), difficult perception of innovations of honey. services (0.6), lack of demand for medical care (0.3), ineffective distribution of time in the provision of honey. services (0.3). ...
The RANEPA Expert and Analytical Center conducted a survey of industry analysts, from which it follows that the main problems of Russian healthcare are the lack of sufficient state control over real practice and the lack of qualified personnel. The lack of funding for the industry ranks only third on the list of problems.
The discrepancy between the set goals and the real state of affairs is the main problem of the Russian healthcare system, analysts of the RANEPA Expert and Analytical Center state in their report. The basis of their work was an expert survey of representatives of the medical professional and managerial community in 2015, 143 people took part in it.
The main problem of the Russian health care system, most of the respondents named the reduced influence and control of modern politics on the real state of affairs in the industry (17.5%). Also, a sufficient number of experts pointed to problems in the personnel industry - a lack of qualified specialists (13%), the presence of problems in personnel policy (the level of salaries and working conditions - 11,%) and poor-quality and degrading training of medical workers (10.4%).
Only 12% of respondents complained about the deficit in financing of the health care system. In addition, among the problems of the industry, experts noted the low quality of the services and drugs provided (8%), the commercialization of the healthcare system (including corruption; 6%), the inaccessibility of some services and drugs (5%), the low level of equipment of medical institutions with the necessary drugs and equipment (3 %) and insufficient introduction of innovations and technologies (2%).
At the same time, despite the complaints about the health care system as a whole, the respondents considered some of the measures carried out recently within the framework of the state program “Healthcare Development” to be effective. The most effective, in their opinion, turned out to be the development of such areas as maternal and child health, improving the provision of emergency medical care, including emergency specialized medical care and medical evacuation, and the introduction of innovative methods for diagnosing diseases. The least effective and requiring additional development were the introduction of the basics of personalized medicine, staffing of the health care system in accordance with modern needs and the provision of palliative care to the population.
The best way to improve the quality of Russian healthcare work, according to the majority of survey participants (49%), could be transferring healthcare workers to an “effective contract” and creating incentives for medical personnel to work. It is also necessary to develop fundamental science in such areas as evidence-based medicine, biostatistics, pharmacoeconomics, economic analysis with the involvement of experts and teachers from other countries, according to 44% of respondents. 43% of experts are in favor of revising the system of indicators reflecting the state of affairs in the health sector (where indicators of life expectancy and mortality are placed on a par with the average salary of doctors), while 34% consider it necessary to create a scientifically based methodology for assessing the effectiveness of budget spending. funds. An independent review system would also help to analyze budget expenditures (41%). The development of entrepreneurial and investment programs aimed at improving the healthcare sector is supported by 40% of the respondents.
1A. A. Belovodsky
The proposed article examines the problems of the Russian healthcare sector. A brief analysis of the main problems is given (low efficiency of healthcare, stagnation of the pharmaceutical industry, high prices for drugs for the population). And also describes the ways to solve them, proposed by both experts and the author of the article.
Introduction
The wealth of any state is its population. People create the state and are the source, the engine of its development and prosperity. But in order to be active, a person must be healthy. Therefore, one of the most important functions of the state is to maintain the health of its population. This support is provided through the health care system.
Health care is a set of measures of a political, economic, social, legal, scientific, medical, sanitary-hygienic, anti-epidemic and cultural nature, aimed at preserving and strengthening the physical and mental health of each person, maintaining his long-term active life, providing him with medical assistance in case of deterioration health.
According to the Constitution of the Russian Federation, "The Russian Federation is a social state" in which "labor and human health are protected." But in practice, everything is far from what it is written.
Most experts agree that the health care system of the Soviet Union was one of the best in world practice, since it performed all the functions assigned to it in terms of quality, availability and provision of medical services, medicines and materials. But after the collapse of the USSR, it entered a phase of stagnation: funding was greatly reduced, highly qualified specialists in the field of medicine went abroad, scientific research in medicine ceased, the production of drugs and devices for diagnosing and treating diseases was greatly reduced.
In the early 2000s, when the situation in the country began to gradually improve, the authorities turned their attention to the healthcare sector. But there are so many accumulated problems that they cannot be solved at once and in a short period of time.
Thus, the most important condition for the further development of the healthcare sector is the transition to an innovative way of development, in connection with which the implementation of the following principles should be ensured:
- government regulation combined with effective competition in the innovation sphere;
- preparation and transition of industry to increase the output of high-tech and science-intensive products that meet the needs of the market and the prospects for its development;
- creation of long-term conditions for increasing labor productivity;
- concentration of resources on innovations that will provide positive structural changes in the economy;
- stimulation of business and investment activity in the field of scientific, scientific, technical and innovation activities through tax, credit and other economic benefits;
- integration of investment, scientific and technical, educational and industrial activities;
- ensuring legal protection of objects of intellectual property and copyright in the dissemination of scientific and technical knowledge and information;
- cooperation of all levels of government, as well as the state, subjects of the federation and municipalities on the issues of modernization and technological renewal of the basic sectors of the economy and the social sphere;
- publicity and discussion of priority innovative programs and projects during open competitions.
It is not without reason that state regulation is placed in the first place among the principles. Without it, innovative development will not work, since private business is reluctant to get involved in the innovation process. Regulation and support in the field of innovation by the state should be as follows:
- development of regulatory legal acts in the field of innovation, organization and control over their implementation;
- determination of priorities in the field of innovation, development and implementation of innovative programs and projects;
- creation of an innovative infrastructure and conditions for innovative activities (incentives through preferential taxation, subsidies, subsidies from budgets);
- formation and placement on a competitive basis of the state order for the creation of science-intensive products and technologies;
- protection of the rights of investors and creditors;
- training and advanced training of personnel employed in the field of innovative activities;
- coordination of actions of subjects of innovation activity;
- support for the creation of subjects of investment activities with the participation of foreign capital, with the provision of appropriate state guarantees for activities.
Thus, the purpose of this essay is to characterize the problems of the healthcare sector in Russia and ways to solve them.
The following tasks were set:
1) a description of the problems in the health sector;
2) a description of the measures taken in Russia to eliminate the problems;
In the abstract, information was used not only from various sources, but also the observations of the author himself.
1. Problems of the Russian healthcare system
First of all, one should dwell on the low efficiency of the entire health care system, which gives rise to the low quality of medical services provided. The reasons for this state of affairs are the following:
1) lack of specialists, medical equipment, hospital facilities, which generates long queues of patients during the opening hours. Doctors have to work in an emergency mode, which automatically reduces the quality of services provided;
2) short admission schedule. Visiting hours often end before 2 pm. Those who did not have time to get to the appointment are forced to come on another day, that is, to take time off from work again, therefore, not to fulfill a number of their duties. Such distraction of employees negatively affects both the company itself (the degree of negative consequences will directly depend on the position of the employee and the possibility of replacing him), and the employee of this company (reduction in wages);
3) inability to timely receive the required medical care. This is a consequence of the lack of specialists, equipment, high cost of medicines and medical services;
4) low qualification of doctors. It often happens that in two different clinics, doctors make different diagnoses for the same symptoms. Accordingly, the treatment does not give the expected effect;
5) absence or aging of medical equipment. In most hospitals, patients are examined and treated using Soviet equipment. And undergoing treatment or examination using new equipment (if any) often costs a lot of money;
6) low wages and lack of mechanisms to stimulate quality work.
The shortage of specialists and hospital facilities is especially noticeable when comparing cities both within one region and between regions. So, if in the regional center or the capital of the republic, most hospitals and clinics have been repaired and have new equipment, then in simple cities, especially remote from the center, there are often few clinics in which people cannot receive the required volume of medical services. How often in the hospitals of the capitals of the subjects of the federation one can see people from other cities and hear about the lack of the necessary apparatus or specialist in their city.
The low efficiency of the health care system strongly “hits” the country as a whole, especially its economy.
The next serious problem is in the area of drug production. The modern population of most countries cannot live without antibiotics, vaccinations, and many different drugs. And if more than 80% of the drugs required for its population are produced domestically, then there are practically no problems. But if the country imports most of the drugs, then there is a "threat to national biological security." Russia also belongs to such countries: imports of medicines make up about 80% of their consumption. Most of the domestic drugs are either Soviet era developments (brought to industrial production) or generics (a drug with proven pharmaceutical, biological and therapeutic equivalence with the original, but not patent protected; that is, it is a copy of the original third-party drug). New developments in this area are funded by the largest companies in the pharmaceutical market (Pharmstandard, Otechestvennye mediciny, Nizhpharm, Veropharm, etc.), while the rest receive grants from abroad and occasionally government orders.
Also, the reasons for the stagnation of the pharmaceutical industry were:
1) the outflow of specialists abroad. The so-called "brain drain" has long become a national disaster in Russia. Scientists move to other countries because they are offered high pay, guaranteed orders and provided with all the necessary research equipment;
2) underinvestment. Pharmacology is a specific area of health care with its own concepts and patterns. Few of the potential investors are able to understand the meaning of the development and assess its prospects. It is also discouraged by the uncertainty of the payback period and the high medical risks of manufactured drugs;
3) the inability of scientists to "sell" their ideas. Russia has always been famous for its people. Today there are groups of enthusiasts developing new drugs. But the matter does not go beyond the idea and the initial developments, since they do not know how to properly present their development to investors in order to further test it and launch it into production;
4) the high cost of developing new drugs. According to experts, investments in the development of a new drug amount to at least $ 600 million. Of this, 10-15% goes to the development of the molecule, 25-30% to preclinical trials in animals, 50-60% to clinical trials in humans. If we are talking about the development of a fundamentally new formula, then the costs for the entire cycle (from research to market launch) can reach more than $ 1 billion;
5) long term. The minimum development time for a new drug is 3 years;
6) insecurity of intellectual property. This problem is not specific to the pharmaceutical industry only. It is typical for Russia as a whole. Only in 2006, the legal framework for the protection of intellectual property began to take shape. In particular, on December 18, 2006, Part 4 of the Civil Code of the Russian Federation, devoted to intellectual property, entered into force;
7) availability of generics. Large modern pharmaceutical companies have little interest in the development of new drugs due to the large number of generic companies. Generics in most cases do not differ in quality and properties from the original, but they cost an order of magnitude cheaper, which reduces the profitability of a new drug from the developer.
A little more detail should be given to the problems of financing drug development. The high cost of the full cycle of drug development (from idea to production) makes such developments impossible for medium and small companies. But they participate in the development as "generators of ideas" or the first stage of research (creation of a drug formula). In the future, they sell their developments, most often, to foreign companies due to the high pay. In addition, according to experts, sometimes domestic companies do not need new developments, which is explained by the lack of funds to continue the development, or the presence of a large number of their own drugs, or the successful release of generics for imported drugs.
Foreign grants are another way of survival for representatives of a medium-sized pharmaceutical business. According to Rosprom's estimates, the average grant is $ 100,000, with 30-50% of Russian companies working on them. Development is carried out until the stage of obtaining the formula, then it is sold abroad.
Also, companies have a chance to receive the necessary funds by contacting special funds. Now entrepreneurs are helped by the Small Business Support Fund, which issues money on the condition that the entrepreneur has a patent. The amount of funds allocated at the earliest stage of development is 1 million rubles. In the future, if it is possible to attract an investor, the Fund will allocate another 3.75 million rubles. Also, there are 3 venture funds operating in the country, and in the future they will establish 7 more. Their capital will be formed at the expense of private and public funds. The money will be given to entrepreneurs on the condition of entering the capital of the company being created and receiving a share of the profit in the future.
Another way to solve the problem of financing is government procurement of drugs and orders. But so far this mechanism is ineffective, since 89% of the required drugs are purchased from foreign companies during government purchases. But the priority should be given to Russian developments.
The next problem associated with drugs is their high cost to the population. No, there is no malicious intent from drug manufacturers (as many people think). This is facilitated by a number of reasons:
1) fluctuation of the ruble exchange rate. Since October 2008, a smooth devaluation of the ruble began in Russia, as a result of which the dollar grew against the ruble by almost 40%, which affected the rise in the cost of imports. And since 80% of the drugs consumed by the residents of the country are imported, the end consumers received the main blow from the devaluation;
2) high cost and duration of development. Therefore, all fundamentally new drugs entering the market are available only to a limited circle of consumers (either the rich, or those to whom the developer company allocated them for free). One example is the modern development of a vaccine against "swine flu" by the British company GlaxoSmithKline Plc. The development of the vaccine took 5 years, more than $ 3.2 billion was spent. The price of the finished vaccine is $ 10. 50 million doses were donated to the World Health Organization. And now let's present a few calculations on how much the imported vaccine against "swine flu" will cost for the population of Russia:
The dollar exchange rate established by the Central Bank of the Russian Federation, as of 13.10.2009 - 29.5 rubles;
The cost of the drug is $ 10;
Import duty on medicines - 10%;
Thus, the cost of this vaccine when crossing the border is 324.5 rubles. (10 * 1.1 * 29.5).
The final cost will consist of retail markups, delivery and promotion costs. It can be assumed that the cost for the population will be about 500 rubles. for 1 dose. It is obvious that the majority of the Russian population will not be able to afford such a vaccine due to low incomes, which increases the risk of morbidity and mortality from the "swine flu" virus.
3) unreasonable prices for medicines. Recently, during a visit to Zelenograd, the problems of the high cost of drugs were raised by V.V. Putin, focusing attention and misunderstanding that foreign medicines are often sold in Russia at prices many times higher than in other countries.
The population is often afraid to buy Russian drugs, preferring imported ones, since there is no confidence in the quality of domestic drugs. In addition, most of the imported drugs have no analogues in Russia.
The same situation (as in the example with calculating the cost) is observed in the pharmaceutical market as a whole, which puts the Russian state under serious threat due to the high risk of morbidity among the population and a decrease in the possibilities for its rapid recovery.
2. Ways to solve health problems
How can Russia get out of such a deplorable situation with health care? The main thing is reforms. But not point-by-point according to the principle "find the decisive link, pull on it - and everything will be resolved." A set of reforms is needed to address all elements of health care. They must be thoughtful and complete, otherwise, as is often the case in Russia, they will only make matters worse.
To improve the efficiency of the healthcare sector, experts propose to develop a mechanism to stimulate competition between physicians and medical institutions. It is required to create a mechanism that will interest medical professionals in improving the quality of their services. For example :
1) creation of a database of doctors and their patients (who are constantly served by him). Such a system operates abroad, where health care is free (USA, Western European countries), and makes it possible to identify highly qualified doctors;
2) provide financing to medical institutions for the effectiveness of the services they provide. That is, the less a person spent within the walls of the hospital, and if he did not have a relapse of the disease, then the medical institution that provided him with assistance will receive more funding than the rest. This mechanism is used in most developed countries (Great Britain, etc.);
3) it is necessary to adopt a number of laws to promote competition in healthcare;
4) it is necessary to change the organizational and legal form of medical institutions. Today they are all state-owned. This means that the resulting financial results from their work go to the state: the surplus of funds is taken away, the arising debts are extinguished. This situation demotivates medical institutions to work effectively. They should be given more freedom in their activities;
5) one should take a differentiated approach to the development of the health sector in different territories of the Russian Federation due to their unequal development. Somewhere it is only necessary to increase the efficiency of healthcare by stimulating competition to develop and improve the quality of medical services, since the region (city) has the necessary medicines, equipment, and specialists. And somewhere, first it is necessary to resolve the issue of the shortage of drugs, medical equipment, specialists, and only then introduce mechanisms to stimulate competition in the healthcare sector.
The issues of remuneration of medical specialists should be approached from the point of view of the development of the region (city), rather than increase wages by the same amount throughout the country. Due to the strong differences in the level of development of the subjects of the Federation, municipalities, the amount of the increase in wages will be perceived differently everywhere. So, in Moscow, 10 thousand rubles. the allowance for the district doctor means very little, and in Dagestan the same amount is a lot of money.
It is also necessary to create mechanisms, thanks to which free medical care would first of all be received by those who have nothing to pay with, and those who have something to pay with, in the presence of a shortage (equipment, specialists, medicines) could pay for the medical care required for themselves.
Another way to develop competition is to use modern information advances in the healthcare sector. In particular, experts propose the idea of creating a personalized database of individual accounts. On its basis, it will be possible to scientifically substantiate the required number of specialized beds in a particular region.
Improving the quality of medical care will also be achieved through the development of intensive care units (intensive care units of various specializations). In the West, each hospital has 20-25% of intensive care beds. In Russia, this figure does not exceed 5%.
The next problem in the healthcare sector - tariffs for medical services - should be resolved through civilized government intervention. Medical rates should include all cost items. They should take into account the required profitability and the level of projected inflation.
To attract funding and stimulate new developments, it is proposed to establish venture funds (with the participation of different capital), to allocate government grants for research. Business cooperation with universities and science cities begins. Today there are biotechnological laboratories on the basis of Moscow State University, Stavropol State University, and a science city in Pushchino. Their task is the first stage of development. In the future, the resulting formula will be sold to a private company.
The state needs to stimulate the innovative development of the entire economy in general and the health sector in particular. As noted earlier, there are practically no new developments in drugs and medical equipment in Russia. To rectify the situation, the state, first of all, needs to develop an innovative infrastructure, change tax legislation (increasing tax incentives and introducing tax holidays for companies carrying out new developments). It is envisaged in the near future to create several scientific research institutes to conduct scientific research in the field of medicine.
But there are already real shifts in this situation. So in 2008 19.4 billion rubles were allocated from the budget. for the construction of new medical technology centers in Penza, Khabarovsk, Astrakhan and other cities. With the support of the state, the medical direction is developing in technoparks (Kurchatovsky, Zelenogradsky, Obninsky), where new methods of treatment, medicines, and equipment are being developed.
In early 2005, the Supplemental Drug Supply program was launched. The essence is the free provision of medicines to privileged categories of the population. For these purposes, funds were annually allocated from the budget for the purchase of medicines. 89% of purchases in monetary terms are from foreign companies. In this regard, experts advise to shift the focus to drugs from domestic manufacturers.
All of the above is what the experts suggest. In general, the author agrees with their suggestions. But after analyzing the problems of the healthcare sector in Russia, he proposes an additional series of measures aimed at improving the situation.
The most important thing is innovative development. The state should become the initiator of the innovation process. It must create incentives for businesses to be motivated to invest in costly, risky projects. To do this, it is necessary to change the legislation in terms of innovative activities of companies. For companies that are developing new drugs or medical equipment, tax breaks should be introduced for the first few years (up to 3 years) of development. In the future, they should reduce their income tax at the stage of promoting a new drug (equipment) on the market. As soon as the volume of sales reaches the targets and continues to grow, such companies should be transferred to the general tax regime.
At the initial stage of development, the state should actively help companies financially, especially young firms with promising developments. To do this, you can use the funds of federal target programs, government orders, grants, the creation of joint ventures with private business, the creation of various venture funds.
To stimulate new developments, it is necessary to create research centers (at least one in each federal district), under the roof of which to gather scientists and provide them with funding for their ideas. In the future, it will be possible to either sell the developments to private companies, or organize their industrial production and market promotion within the framework of joint ventures, or use the rental or leasing form of the development implementation. When selling a development, the contract should specify the forms and terms of payment. Optimal would be a step-by-step payment (initial payment, then fixed or percentage deductions from the proceeds from the sale of a new drug / equipment). With the lease form, the acquirer (lessee) will only pay royalties for the use of the formula or industrial design of the device without transferring ownership of the leased development. Moreover, this development can be leased to other companies. In the case of a leasing form, the acquirer (lessee) will use all the advantages of the leasing scheme.
To facilitate the transition to an innovative path of development, it is initially possible to create generics based on Western samples, but on their basis to produce our own developments. But it is necessary to strengthen control over generics, which will automatically increase public confidence in them and reduce the number of side effects.
To have the opportunity for innovative development, highly qualified personnel are needed. It is necessary to look for and encourage talented students, to involve them in work in research projects. It is also necessary to stop the outflow of domestic scientists abroad. For this, it is necessary to create all the conditions for their research activities: to provide laboratories, to allocate funding. But such measures should be taken in priority scientific areas, as well as promising areas. Do not waste resources on dubious research (of which you can find many in the modern world).
One of these key areas (in addition to the use of nanotechnology in medicine, the creation of new drugs and medical equipment) should be diagnostics. The development of this area of medicine will significantly reduce the duration of treatment and the number of patients of moderate and high severity, since it will be possible to identify and treat diseases at an early stage, when it is much easier to do than later.
To solve the problem of the cost of drugs, the pricing should be monitored along the entire chain (from the manufacturer to the retailer). And to punish those who unreasonably raise prices.
Conclusion
Based on the results of the work carried out, it can be concluded that, despite the huge volume of accumulated problems, the Russian health care system is beginning to change towards improvement.
But there is another serious problem that cannot be solved only with new ideas and funding. This problem is not highlighted by experts, but every person faces it. We are talking about consumer confidence in Russian medicines, medical equipment, and doctors. And the reason for the named problem lies precisely in those flaws in the health care sector, named in the work. In addition, since Soviet times, people have had the idea that all imported goods have better quality, characteristics, and are safer than Russian counterparts (if any).
Lost trust is always very difficult to regain. But if all the problems identified in the work are solved, if their solution does not drag on for a long time, then people will switch to domestic drugs and medical equipment, they will cease to consider the maximum withdrawal of money from the patient as the main goal of doctors. The number of days spent in hospitals will be reduced. Mortality will decrease and life expectancy will increase. All this will immediately have a positive effect on the country's economy. Only then will it be possible to say that the Russian healthcare system is effective.
BIBLIOGRAPHY
1. Russian Federation. Constitution (1993). Constitution of the Russian Federation [Text]: official text.
2. Russian Federation. The laws. Customs Tariff of the Russian Federation [Text]: Approved by the Decree of the Government of the Russian Federation of November 27, 2006 N 718.
3. Impudent, N. Economy and health care [Electronic resource] / N. Impudent // http://medreforma.narod.ru/Economic.html
4. Nepomniachtchi, A. 2025: Spaceship in a tablet [Text] / A. Nepomniachtchi // SmartMoney. - 2008. - No. 32 (122).
5. Sovinsky, M. The rules of drug control [Text] / M. Sovinsky // Energy Money. - 2007. - No. 39 (645).
6. Fillipenko, E. Medicine for pharmacists [Text] / E. Fillipenko // Energy of industrial growth. - 2007. - No. 1-2.
7. Sidibe, P. How to cure a pharmacy [Text] / Sidibe P. // Rossiyskaya Gazeta. - 12.10.2009. - No. 5016 (192).
8. IFX-NEWS Glaxo can earn more than $ 4 billion from the "swine flu" vaccine. [Electronic resource] / IFX-NEWS // http://finansmag.ru/news/39457
9. Emelianenko, E.B. Features of investing in medicine [Electronic resource] / Ye.B. Emelianenko // http://medinfa.ru/
article / 99/115329 /
10. Emelianenko, E.B. How to raise funds for the development of medical innovations? [Electronic resource] / E.B. Emelianenko // http://marketing.rbc.ru/articles/10/03/2009/562949955897116.shtml
11. Leibin, V. Diagnosis of medical reform: a grave condition [Electronic resource] / V. Leibin // http://www.polit.ru/
country / 2004/01/15 / medevent.html
12. Russian medicine: ethics and economics [Electronic resource] / Interview with Lev Yakobson // http://www.polit.ru/
analytics / 2005/10/03 / med1.html
Bibliographic reference
A. A. Belovodsky HEALTHCARE IN RUSSIA: PROBLEMS AND WAYS OF SOLUTION // Modern science-intensive technologies. - 2009. - No. 11. - S. 21-27;URL: http://top-technologies.ru/ru/article/view?id=25977 (date accessed: March 24, 2020). We bring to your attention the journals published by the "Academy of Natural Sciences"
Introduction
1. The concept and history of the formation of healthcare in Russia
1.1 Concept of health care
2.3 Inconsistency of legal regulation of the healthcare sector
3.2 Ways of solving problems of public administration in the field of health care
1.2 History of the formation of healthcare in Russia
Late 17th - early 18th century became a significant time in the history of Russia. The reforms of the outstanding statesman and military leader, the talented and energetic Peter I, made it possible to overcome the cultural self-isolation of Russia (which, however, was never absolute), to open a “window to Europe”, to establish contacts and exchange, to join the common European culture and civilization. Peter's reforms, the exertion of the popular forces, the labor of all of Russia helped in many respects to eliminate the backwardness of the state, played a huge role in the development of the country's productive forces, its industry and agriculture, science and culture. As the great Pushkin wrote about this time, "there was that troubled time when young Russia, straining her strength in struggles, matured with the genius of Peter" 1. Russian medicine was also gaining strength and experience.
Peter I was an educated person, highly valued science. According to the famous historian V.O. Klyuchevsky, he was imbued with faith “in the miraculous power of education” and “reverent cult of science” 2. What is especially characteristic, Tsar Peter, according to his contemporaries, had a genuine passion for medicine. When in 1697 he visited Holland and England as part of the Great Embassy, under the name of the sergeant Peter Mikhailov, he got acquainted there with medical clinics and anatomical laboratories.
They say that Peter listened to the lectures of professor of anatomy Ruysch, was present during operations, and when he saw in his anatomical office a perfectly dissected corpse of a child who smiled as if alive, he could not resist and kissed him (later Peter bought the anatomical collection of Professor Ruysch, she was in St. Petersburg, in the Kunstkamera and the Academy of Sciences).
In Holland, Peter I met with the famous naturalist, one of the founders of scientific microscopy, Anthony van Leeuwenhoek, who, at the request of the king, arrived on his ship. The Dutch scientist “had the honor, besides his other rare discoveries, to show the Emperor, to his great delight, the amazing circulation of blood in the tail of an eel with the help of his special magnifying glasses; thus, two hours passed in various observations, and, leaving, the king shook hands with Levenguk and expressed his special gratitude for the opportunity to see such unusually small objects ”3.
There is a legend that in Leiden he also looked into the anatomical theater to the famous professor Boerhave, a medical luminary of that time, saw how the professor "separated" the corpse and "told" its parts to the students, and then examined the richest collection of preparations, embalmed and "in alcohol ". By the way, having noticed that some of the retinue accompanying him expressed disgust for the dead body, Peter became very angry and forced them to tear apart the muscles of the corpse with their teeth.
“The spread of medicine in our country under Peter the Great was greatly facilitated by the monarch’s passion for anatomy and surgery,” noted the historian of medicine N. Kupriyanov later. - ... In surgery, the emperor acquired many knowledge and even practical skills. As a rule, the monarch carried two sets with him: one with mathematical, the other with surgical instruments and loved surgery so much that under the leadership of Termont (this surgeon came to Russia during the reign of Tsar Alexei Mikhailovich - MM) methodically opened corpses, made incisions, bleeding , bandaging wounds and pulling out teeth. The tsar ordered to report on every more interesting operation performed in a hospital or a private house. The monarch not only watched the operations, but did them himself. "
A skilled craftsman, Peter knew many crafts perfectly. Success in this instilled in him a strong confidence in the sleight of his hands: he really considered himself both an experienced surgeon and a good dentist. It used to be that close people suffering from any ailment that required surgical help were horrified at the thought that the tsar might find out about their illness and, having appeared with instruments (Peter I had his own surgical instruments, which included a pair of lancets, knife, pliers for pulling teeth, scissors, a probe for wounds, etc.), would offer his services as a surgeon: of course, it was impossible to refuse the king, but it was also impossible to trust him as an operator, as a doctor, as a healer. Still, as they say, after him there was a whole sack with his teeth pulled out - a monument to his dental practice.
During the reign of Peter I, which in fact opened the history of Russia in the 18th century, the state character continued to be a distinctive feature of the organization of medical business in the country. Despite the difficulties associated with large-scale reforms, the state tried to take care of the health of its citizens, especially the military, spending certain amounts from the budget and managing all medicine in the country.
It is known that during the reign of Peter I, large military hospitals were opened in Russia - in Moscow (1707), Petersburg (1716), Kronstadt (1720), Revel (1720), Kazan (1722), Astrakhan (1725) and other cities of the country. ... By a decree of Peter I (1721), magistrates undertook to build "zemstvo dependent state hospitals for the charity of the orphan, the sick and the disabled and for the elderly people of both sexes": as a result, 10 hospitals and over 500 infirmaries were created in the country during his lifetime. In 1715, when he laid the foundation for a naval (Admiralty) hospital in St. Petersburg, on the Vyborg side, Peter I said: “Here the exhausted man will find help and comfort, which he has lacked until now; God only grant that many never need to be brought here! "
It should be emphasized that it was Peter I who provided state support to the measures taken by the Orthodox Church and many of its monasteries to combat "foundlings" and to help orphans and illegitimate children; he especially actively supported the initiatives of the Novgorod Metropolitan Job. Back in 1706, Metropolitan Job, using the monastic income, opened three hospitals on the banks of the Volkhov River, as well as a house for passers-by and "a house for illegitimate and all kinds of thrown babies." For this "home of thrown babies" a whole monastery in Kolmov was allocated. A. Gorchakov in his book "Monastic Order" (1863) reports that Metropolitan Job in 1714 had "10 strangers, 15 beggars or hospitals and a house for foundlings."
The highly useful activity of Metropolitan Job Peter often cited as an example not only to the hierarchs of the Church, but also to his closest circle: Christian charity was becoming an important state affair. Moreover, in a decree of January 16, 1712, Peter I directly prescribed: "In all the provinces, make tapestries for the crippled, as well as unseen reception and feeding of babies who were born of illegitimate wives, following the example of the Novgorod arch-father."
In another tsar's decree, it was emphasized: “In the same way, about the same things, the blessed Job, Metropolitan of Novgorod, made a thorough and soul-saving examination of the same deeds in Veliky Novgorod, to choose skillful wives to preserve the shameful babies whom wives and girls give birth to illegally ... Announce the decree so that such babies are not swept away to obscene places ... "
Even in the notebooks of Peter I there are notes indicating that he paid great attention to these undertakings. For example, here is a note made by Peter I at one of the sessions in the Senate:
“Was it done according to the decree on lifting babies, as the Novgorod arch-father Job had. And if not done - why. "
The developing medicine required the expansion of the supply of medicines to the population. Therefore, much attention has been paid to increasing the number of pharmacies. State pharmacies were opened in St. Petersburg, Kazan, Glukhov, Riga and Revel in 1706, and in some other cities - garrisons. At the same time, measures were taken to encourage the creation of free (private) pharmacies.
In 1701, a decree was issued that any Russian or foreigner who wishes to open a free pharmacy with the permission of the government will receive a place without money for this and a letter of gratitude for the hereditary transfer of his institution; such pharmacists were given the right to freely prescribe all the necessary materials from abroad. In Moscow, in addition to two state-owned, it was allowed to open eight more pharmacies. And from 1721, free pharmacies began to open in St. Petersburg and other provincial cities. It is characteristic that both the permission to open pharmacies and control over their activities were in the sphere of state interests. State medicine, primarily the military medical service, required more and more doctors. At first they were recruited abroad. For example, only in 1698 in Amsterdam, along with captains, gunners, navigators and other specialists, were hired, along with captains, gunners, navigators and other specialists, in Amsterdam: each was entitled to a salary of 12 efimks, 13 altyns and 2 money per month10. All these doctors studied medicine not at universities, but as individual apprenticeships with other, more experienced doctors, and then served in the troops or on ships of various European countries.
To find their own, more qualified doctors, it was necessary to train their own doctors in the country, opening special educational institutions for this purpose. And in the 18th century, after the first hospital school in Moscow, several more schools were opened. Pupils of hospital schools, who were equally competent in therapy and surgery, were sent primarily to the army and the navy.
It is generally recognized that economic progress and the associated political and cultural transformations inevitably determine the need for the rapid development of science. So it was in our country.
Already at the beginning of the 18th century. a school of mathematical and navigational sciences (1701), artillery schools (1701), an engineering school (1713), a naval academy (1713), mining and industrial craft schools (1719) and a number of others appeared in Russia: the St. Petersburg Academy of Sciences (1725), and then and Moscow University (1755). Among the first in Russia, a medical-surgical (hospital) school was opened and trained doctors.
It is important to emphasize that this school represented a fundamentally new type of higher medical educational institutions. The main thing is that, unlike the one that existed in the 17th century. the medical school of the Apothecary Prikaz, which was discussed above, and the first, and all other Russian medical and surgical schools were created only on the basis of large medical institutions - hospitals, which is why at first they were called "hospital".
From the very beginning, the establishment of large, general (i.e. educational) hospitals pursued a twofold goal - the treatment of patients and the teaching of medicine. “The institution of hospitals has a double intention and fruit,” the General Regulations on Hospitals, approved in 1735, legitimized: the first and which has the authority to be - the use of suffering patients, the second - the production and approval of doctors and healers to great art; for the sake of this intention, although in the beginning, physicians and healers should be provided. "
The hospital schools created in Russia were fundamentally different from the medical educational institutions that existed in Western Europe - the medical faculties of universities. As you know, their graduates - doctors of a therapeutic profile - received mainly theoretical education. In contrast, surgeons who did not have a university medical education received practical training in the "craft apprenticeship" method and were considered second-class physicians. However, life showed - and at the beginning of the XVIII century. it became more and more evident that physicians should be well trained in both internal medicine and surgery.
In Russia, where the antagonism between doctors and surgeons inherent in Western Europe never existed, from the very beginning of higher medical education they began to train doctors who were equally competent in surgery and in internal medicine. Higher medical education began in Moscow.
On May 25, 1706, a decree of Peter I was published on the organization of the Moscow "gof-shpital": it should have been built "across the Yauza River, opposite the German settlement, in a decent place ... for the treatment of sick people." The decree emphasized: “And that treatment will be for Dr. Nikolai Bidloo, and two doctors Andrei Repken, and the other, who will be sent; yes, from foreigners and Russians from all ranks of people to recruit 50 people for the pharmaceutical (ie, medical. - MM) science; and for the building and for the purchase of medicines, and for all sorts of things belonging to that, and for the doctor, and doctors, and disciples for the salary, keep money from the fees of the Monastic Order. "
Initially, several wooden two-storey outbuildings were built for the hospital - as they were then called, “houses with light rooms”. The hospital buildings were surrounded by a garden in which medicinal plants were planted.
On November 21, 1707, the hospital was opened, patients began to be admitted here for treatment. “All-merciful sovereign,” wrote the head of the hospital, Dr. Bidloo to Peter I, “your royal majesty was pleased to have ordered the hospital at Yauza to be built, which, with God's blessing, under the care of his Excellency Count Musin-Pushkin (at that time the manager of the Monastic Order. - MM) On November 21, 1707, he was brought into such a state that with it in God's name the beginning was made, and for the first time several sick people were brought into that house ”.
At the same time, the first in the country Moscow hospital (medical-surgical) school began to operate, its first students began to study. On the maintenance of the hospital and the school, the Monastery Prikaz (and then the Holy Synod that replaced it) spent part of the funds received by the clergy from the monastic estates, from fees from the "crown memorials" (they were paid at marriage), from "hospital money" (a kind of tax on medicines collected from all government officials), from “fines money” (for more than a year overdue spiritual confession).
To study at school, knowledge of the Latin language was required - teaching was carried out in this traditional international language of science, so the school initially enrolled students of the Moscow Slavic-Greek-Latin Academy and theological seminaries. These were young people of democratic origin, people from the lower strata of society, primarily from the petty clergy, from the townspeople and artisans, from the Cossacks and soldiers; there were also medicinal children among them. The majority were "natural Russians", but there were also children of foreigners. Forced to achieve everything by their own labor, they looked at learning as labor and for the most part did it with great willingness.
However, not all of those who entered the Moscow hospital school completed the full course of study. So, in 1712, Dr. Bidloo wrote to Peter I: “I took in different years and numbers 50 people before surgical science, of whom 33 remained, 6 died, 8 fled (from schools then, as V.O. Klyuchevsky wrote, very many young people. - MM), 2 were taken to school by decree, 1 for intemperance was sent to the soldiers. " According to age, duration of schooling and success in learning, all students were divided into three articles (categories) - the first, second and third. All of them studied for free and were on full boarding with the state, lived at the hospital in separate rooms, had a common table, received uniforms and a salary. The salary was 1 ruble a month, cloth for a caftan, a camisole and trousers was issued for uniforms - 7 yards each for two years: the quality of the cloth given out depended on the article in which the student consisted.
Initially, there was no fixed period of study at the Moscow hospital school - depending on the student's success, it ranged from 5 to 10 years. The training program provided for a thorough acquaintance with the subjects that then constituted the basis of medical and surgical education. These were, firstly, anatomy, and secondly, "Materia Medica", which included pharmacognosy (systematic botany), pharmacology and pharmacy, thirdly, internal diseases and, fourthly, surgery with desmurgy.
Anatomy, then the most important discipline in medical education, was taught by Bidloo himself.
Nikolai Bvdloo, or, as they called him in Moscow in the Russian manner, Nikolai Lambertovich Bidloo, was born in Holland, in Amsterdam, around 1670. His father Lambert Bidloo was a pharmacist and botanist, a member of the Amsterdam Medical Society, and his uncle Gottfried Bidloo - an anatomist and surgeon - at one time was the life-doctor of the English king, and then - a professor and rector of the famous "Leiden-Batavian Academy". Nikolai Bidloo graduated from this academy, in 1697 he defended his dissertation on the topic "On delayed menstruation" and until 1702 was engaged in medical practice in Amsterdam. The Russian envoy to Holland, Count A.A. Matveev, by order from St. Petersburg, invited Bidloo to Russia as a physician-in-chief of Peter I and signed a corresponding contract with him. In 1702 Bidloo came to Russia, which became his second homeland: he lived here for more than 30 years and died in Moscow in 1735.
For several years Bidloo was the physician of Peter the Great: his duties included constantly accompanying the tsar on his extremely frequent trips to Russia. In addition, Bidloo carried out numerous assignments of the king, who was always interested in medicine.
In Leipzig at the beginning of the 18th century. the magazine "European rumor" was published, which covered the most important political events, the court chronicle was printed, etc. Among the important news from Moscow, "European rumor" published a message that "an anatomical theater has been built in Moscow, which is entrusted to the supervision of Dr. Bidloo, a Dutch and the royal physician; he often anatomizes the bodies of those who have died by ordinary death, and those who have died from wounds, and the king himself is often present with the nobles, especially when doctors are consulted about the properties of the body and the causes of various diseases. "
However, numerous duties began to weigh on Bidloo, and he turned to the king, who was well pleased with him, who, moreover, for health reasons did not need the services of a physician, with a request to give him another service. So Bidloo became the chief doctor of the Moscow hospital and director of the hospital school, where he taught anatomy and other basic subjects.
Particular attention was paid to the study of anatomy at the Moscow hospital school: knowledge of this science was mandatory for surgeons. "To surgery," taught future doctors Dr. Bidloo, "are related so that the surgeon knows: 1. Anatomy, which is the knowledge of the whole human body from the outside and from the inside." A similar anatomical (and later anatomical and physiological) approach, which was widely developed not only in Moscow, but also in other hospital schools, became a pattern that distinguished Russian surgery and medicine in the 18th-19th centuries.
The discipline "matter of medicine" (or, in other words, pharmaceutical science) was taught to the students of the hospital school by the hospital's pharmacists Christian Eichler, and then by Ivan Maak. The hospital had its own garden of medicinal plants (the so-called pharmaceutical garden): in the summer and autumn, the students, together with the pharmacist, went out of town, in the vicinity of Moscow, to collect medicinal plants and replenish the hospital pharmacy.
Since complex medicines then dominated medical practice - tinctures, elixirs, decoctions - from many different ingredients (sometimes from 20-30), students had to write down a large number of long recipes and store them for a long time. They were also given an idea about the then known pharmacopoeias, especially the so-called London one. Along with medicinal plants, students were taught to use for treatment such exotic, but used medicines as dog and fox fat, wolf teeth, antler, hare ankles, etc.
Internal medicine (or simply medicine) included private pathology and therapy. Their study was initiated by Dr. Bidloo.
Bidloo himself taught surgery to the students of the hospital school - only desmurgy ("the establishment of bandages") was taught by his assistant, the doctor Repken, and the doctor Fyodor Bogdanov.
Thus, the training program for future doctors at the Moscow hospital school was very rich, in no way inferior, and in some way superior to the programs of medical faculties of the then Western European universities, in most of which the deadening spirit of medieval scholasticism still dominated. The main thing, of course, was in the practical training of future doctors, in teaching students at the patient's bedside, in the hospital ward.
The glorious time of the reforms of Peter I had a beneficial effect on Russian medicine. As a matter of fact, it is to Peter I that Russian medicine owes much to the fact that in the 18th century. it developed mainly like medicine in other European countries, on the basis of science and thoughtful recommendations, whether it concerned the training of doctors, or the fight against epidemics, or the activities of the military medical service. At the same time, a distinctive feature of Russian medicine continued to be its state character.
The training of medical personnel was carried out in hospital schools (since 1707), medical-surgical schools (since 1786), and since 1798 - in the St. Petersburg and Moscow medical-surgical academies. In 1725 the St. Petersburg Academy of Sciences was opened, and in 1755 the first in the country Moscow University with a medical faculty was created.
An outstanding contribution to health protection was made by MV Lomonosov, who, in his work “The Word on the Reproduction and Preservation of the Russian People,” gave a deep analysis of health care and proposed a number of concrete measures to improve its organization.
In the first half of the 19th century. the first scientific medical schools are formed: anatomical (P.A.Zagorsky), surgical (I.F.Bush, E.O. Mukhin, I.V.Buyalsky), therapeutic (M.Ya. ... NI Pirogov creates topographic anatomy and military field surgery, in which he put forward the position on the importance of organizing medical care during hostilities, emphasized the extremely high role of preventive medicine. NI Pirogov was the first in the world in military field conditions to use ethyl ether for anesthesia (1847), developed many methods of surgical treatment, which are still classical today, and was the first in the country to use female labor in war (1853).
2. Analysis of the national project to improve health management
2.1 New in Russian healthcare legislation
From 01.01.05 the Federal Law "On Amendments to the Legislative Acts of the Russian Federation and the Recognition of Invalidation of Certain Legislative Acts of the Russian Federation in Connection with the Adoption of Federal Laws" On Amendments and Additions to the Federal Law "On General Principles of Organization of Legislative (Representative ) and the executive bodies of state power of the constituent entities of the Russian Federation "and" On the general principles of organizing local self-government in the Russian Federation "dated 22.08.04 No. 122-FZ. In accordance with this law, amendments have been made to 196 legislative acts, including 10 federal laws in the field of public health protection.
The bulk of the amendments were introduced in order to delimit powers between federal government bodies, government bodies of the constituent entities of the Russian Federation and local government bodies, which radically changed the entire system of interbudgetary financial relations within the Federation, including health financing.
In accordance with Art. 35 of the new law, amendments were made to the Fundamentals of Legislation of the Russian Federation on the Protection of Citizens' Health dated July 22, 1993 No. 5487-1.
In the article defining the powers of federal government bodies in the field of health protection (Article 5), the articles defining the powers of government bodies in establishing the structure, organization and operation of federal government bodies of the state health care system were declared invalid. Also from the Fundamentals, the powers to determine the share of health care costs in the formation of the federal budget, trust funds intended to protect the health of citizens, the definition of tax policy (including benefits on taxes, fees and other payments to the budget) in the field of health protection are excluded. This is due to the fact that the structure and procedure for the organization and activities of federal executive bodies are regulated by the Federal Constitutional Law "On the Government of the Russian Federation" and cannot be regulated by special legislation on the protection of the health of citizens. The formation of the federal budget and tax policy are determined by the Budget and Tax Codes of the Russian Federation and also cannot be regulated by special legislation on health protection.
The powers of federal government bodies to determine the nomenclature of specialties in health care have been supplemented by the powers to determine the nomenclature of organizations in health care. This is due to possible changes in the legislation on the organizational and legal forms of organizations, including healthcare organizations, in the near future.
The powers to establish benefits for certain groups of the population in the provision of medical and social assistance and drug provision have been excluded. These and all subsequent exceptions to the legislation of benefits for various categories of the population are associated with "bringing the system of social protection of citizens who enjoy benefits and social guarantees and who are provided with compensation, in accordance with the principle of delineation of powers between federal government bodies, government bodies of the constituent entities of the Russian Federation and bodies of local self-government, as well as the principles of the rule of law with a socially oriented market economy "(preamble of the law).
In our opinion, the powers to issue permits for the use of new methods of prevention, diagnostics and treatment, new medical technologies, have been introduced into the powers of the federal bodies of state power, in our opinion. Previously, these powers belonged to the powers of the constituent entities of the Russian Federation.
Part 2 of this article was declared invalid, and therefore, in accordance with the current legislation, today certain powers in matters of protecting the health of citizens cannot be transferred by the Russian Federation to the constituent entities of the Russian Federation and the constituent entities of the Russian Federation cannot transfer their powers to the Russian Federation. This is consistent with the concept of the law on a strict delineation of powers between federal government bodies, government bodies of the constituent entities of the Russian Federation and local government bodies.
In the article defining the powers of the bodies of state power of the constituent entities of the Russian Federation (Article 6), a number of powers of the bodies of state power of the constituent entities of the Russian Federation are set out in a new edition, which led to a change in the content of powers. The powers of the bodies of state power of the constituent entities of the Russian Federation include the development and implementation of programs for the development of health care, prevention of diseases, the provision of medical care, medical education of the population and other issues in the field of protecting the health of citizens; establishment of the structure of the governing bodies of the state healthcare system of the constituent entities of the Russian Federation, the procedure for their organization and activities; development of healthcare institutions in the constituent entities of the Russian Federation; their material and technical support; control over compliance with the standards of medical care in the manner prescribed by the legislation of the Russian Federation and the legislation of the constituent entities of the Russian Federation; the formation of expenditures of the budgets of the constituent entities of the Russian Federation for health care in terms of the provision of specialized medical care in dermatovenerologic, anti-tuberculosis, narcological, oncological dispensaries and other specialized medical organizations in accordance with the nomenclature of medical organizations approved by the authorized federal executive body (with the exception of federal specialized medical organizations , the list of which is approved by the Government of the Russian Federation), including the provision of medical organizations with medicines and other means, medical devices, immunobiological preparations and disinfectants, as well as donor blood and its components within the framework of the Program of state guarantees for the provision of free medical care to citizens of the Russian Federation, compulsory medical insurance of the non-working population, the provision of specialized (sanitary and aviation) with bark of medical care; development and approval of territorial programs of state guarantees for the provision of free medical care to citizens of the Russian Federation, including territorial programs of compulsory medical insurance; establishing the order and volume of social support measures provided to certain groups of the population in the provision of medical and social assistance and drug provision.
Thus, the establishment of the order and volume of measures of social support (in the old terminology - benefits) provided to certain groups of the population in the provision of medical and social assistance and drug provision under the current legislation is now the authority of the constituent entities of the Russian Federation. As a result, from 2005 the regions will have to finance all their obligations, including those for preferential payments. Having strictly delineated the powers in matters of social support with the subjects of the Federation, the federal center assigned responsibility for possible social problems to the regions.
The powers to issue permits for the use of new methods of prevention, diagnosis and treatment, new medical technologies, licensing of medical and pharmaceutical activities in the territories of the constituent entities of the Russian Federation have been removed from the powers of state authorities of the constituent entities of the Russian Federation.
Part 2 of the article on the transfer of the powers of the state authorities of the constituent entities of the Russian Federation in matters of health protection to the state authorities of the Russian Federation was declared invalid.
The jurisdiction of local government bodies (Art. 8), in accordance with the amendments, includes control over compliance with legislation in the field of public health protection; protection of human and civil rights and freedoms in the field of health protection; formation of governing bodies of the municipal health care system; development of institutions of the municipal health care system, determination of the nature and scope of their activities; creating conditions for the development of a private health care system; organization of primary health care in outpatient polyclinic, inpatient polyclinic and hospital institutions, including the provision of these medical organizations with medicines and other drugs, medical products, immunobiological preparations and disinfectants, as well as donor blood and its components, medical care for women in the period of pregnancy, during and after childbirth and emergency medical care (with the exception of air ambulance), ensuring its availability, monitoring compliance with standards of medical care, providing citizens with medicines and medical products in the jurisdictional territory; environmental protection and environmental safety.
It should be noted that the organization and financing of specialized medical care in municipal health organizations did not fall under the authority of the state authorities of the constituent entities of the Russian Federation, or the authority of local self-government bodies.
A number of changes concern the organizational aspects of healthcare activities in the Russian Federation.
In accordance with the new law, the state health care system (Article 12) includes federal executive bodies in the field of health care, executive bodies of the constituent entities of the Russian Federation in the field of health care, the Russian Academy of Medical Sciences, which, within their competence, plan and implement measures to protect health. citizens.
The state health care system also includes state-owned and subordinate to the management bodies of the state health system medical and preventive and research institutions, educational institutions, pharmaceutical enterprises and organizations, pharmacies, sanitary and preventive institutions, territorial bodies established in accordance with the established procedure for implementation of sanitary and epidemiological surveillance, forensic medical examination institutions, logistics services, enterprises for the production of medicines and medical equipment and other enterprises, institutions and organizations.
The state health care system includes medical organizations, including medical and preventive institutions, pharmaceutical enterprises and organizations, pharmacies created by federal executive bodies in the field of health care, other federal executive bodies and executive bodies of the constituent entities of the Russian Federation.
Art. 13. Municipal health care system - set out as follows.
The municipal health care system can include municipal health authorities, as well as municipal-owned medical, pharmaceutical and pharmacy organizations that are legal entities.
Municipal health authorities are responsible within their competence.
Financial support for the activities of organizations of the municipal health care system is an expenditure obligation of the municipality.
The provision of medical care in organizations of the municipal health care system can be financed from the funds of compulsory medical insurance and other sources in accordance with the legislation of the Russian Federation.
Art. 14. Private health care system - set out as follows.
The private health care system includes medical and prophylactic and pharmaceutical institutions, the property of which is in private ownership, as well as persons engaged in private medical practice and private pharmaceutical activities.
The private health care system includes medical and other organizations created and funded by legal entities and individuals.
A number of changes concern the rights of citizens in the field of health care.
Part of Art. 20, according to which, in case of illness, citizens had the right to 3 days of unpaid leave during the year without presenting a medical document. This part came into conflict with the Labor Code of the Russian Federation.
Part 5 of Art. 23. The rights of pregnant women and mothers are set out as follows.
"The procedure for providing full nutrition to pregnant women, nursing mothers, as well as children under the age of 3, including through special food outlets and shops at the conclusion of doctors, is established by the legislation of the constituent entities of the Russian Federation." Thus, the provision on state guarantees for the provision of adequate nutrition to pregnant women, lactating mothers and children under 3 years of age has been excluded.
In Art. 24. The rights of minors - it is determined that dispensary observation and treatment in children's and adolescent services is carried out in the manner established by the federal executive body in the field of health care, and on conditions determined by the state authorities of the constituent entities of the Russian Federation. The right to medical and social assistance and food on preferential terms is excluded. Responsibility for exercising the right to free medical advice in determining professional suitability has been transferred to the constituent entity of the Russian Federation (minors have the right to "free medical consultation when determining professional suitability in the manner and under the conditions established by the state authorities of the constituent entities of the Russian Federation). Minors with physical or mental disabilities. at the request of parents or persons replacing them, they can be held in social protection institutions in the manner and on conditions established by the state authorities of the constituent entities of the Russian Federation (instead of "at the expense of budgets of all levels") ". Thus, the federal bodies of state power have no powers to exercise the rights of minors. All responsibility for the realization of the rights of minors lies with the constituent entity of the Russian Federation and depends on the availability of money in the budget of this constituent entity of the Russian Federation.
The right to receive medical care in the institutions of the municipal health care system is excluded from the rights of military personnel (Article 25), which will lead to an even greater problem in the provision of medical care to this category of citizens.
Recognized as invalidated by Art. 26. The rights of elderly citizens; Art. 27. The rights of persons with disabilities; Art. 28. The rights of citizens in emergency situations and in ecologically unfavorable areas.
It is assumed that the rights of these groups of the population should be enshrined in special laws.
Changes have been made to section VIII. Guarantees for the implementation of medical and social assistance to citizens.
Art. 38. Primary health care - is set out as follows.
Primary health care is a basic, affordable and free type of medical care for every citizen and includes the treatment of the most common diseases, as well as injuries, poisoning and other emergency conditions; medical prevention of major diseases; sanitary and hygienic education, other activities related to the provision of health care to citizens at the place of residence.
Primary health care is provided by the institutions of the municipal health care system. Institutions of public and private health systems can also participate in the provision of primary health care on the basis of contracts with health insurance organizations.
The volume and procedure for the provision of primary health care is established by legislation in the field of public health protection.
The financial support of measures for the provision of primary health care in outpatient polyclinic, inpatient polyclinic and hospital institutions, medical care for women during pregnancy, during and after childbirth in accordance with these Fundamentals is an expenditure obligation of the municipality.
The provision of primary health care can also be financed from compulsory health insurance and other sources in accordance with the legislation of the Russian Federation.
Art. 39. Ambulance - set out as follows.
Emergency medical care is provided to citizens in conditions requiring urgent medical intervention (in case of accidents, injuries, poisoning and other conditions and diseases); obliged to provide it in the form of first aid by law or by a special rule.
Emergency medical care is provided by emergency medical institutions and units of the state or municipal health care system in accordance with the procedure established by the federal executive body in charge of legal regulation in the field of health care. Emergency medical care for citizens of the Russian Federation and other persons on its territory is provided free of charge.
Financial support of measures for the provision of specialized (sanitary and aviation) emergency medical care in accordance with these Fundamentals is an expenditure obligation of the constituent entities of the Russian Federation.
Financial support of measures for the provision of emergency medical care (with the exception of sanitary and aviation) to citizens of the Russian Federation and other persons located on its territory, in accordance with these Fundamentals, is an expenditure obligation of the municipality.
The right to free ambulance medical care was excluded in the draft law of the Government of the Russian Federation, and it was with great difficulty that it was defended and preserved.
Art. 40. Specialized medical care - is set out in the following edition.
Specialized medical care is provided to citizens for diseases requiring special diagnostic methods, treatment and the use of complex medical technologies.
Specialized medical care is provided by specialist doctors in medical institutions that have received a license for the specified type of activity.
The types and standards of specialized medical care provided in health care institutions are established by the federal executive body in charge of legal regulation in the field of health care.
Financial support of measures for the provision of specialized medical care in dermatovenerologic, anti-tuberculosis, narcological, oncological dispensaries and other specialized medical organizations (except for federal specialized medical organizations, the list of which is approved by the Government of the Russian Federation) is an expenditure obligation of the constituent entities of the Russian Federation.
Financial support of measures for the provision of specialized medical care provided by federal specialized medical organizations, the list of which is approved by the Government of the Russian Federation, in accordance with these Fundamentals, is an expenditure obligation of the Russian Federation.
Within the meaning of the article, specialized medical care is provided only in institutions of the state health care system (federal specialized medical organizations or specialized medical organizations of the constituent entities of the Federation), which is incorrect. Specialized medical care is also provided in municipal health care organizations (both outpatient and inpatient). Accordingly, the law does not contain a clause on the financial support of measures for the provision of specialized medical care in municipal health care organizations.
Thus, primary health care will be provided only at the level of the municipality, and specialized, including in municipal health organizations, if any (with the exception of federal specialized medical organizations, the list of which is approved by the Government of the Russian Federation), in accordance with by these Fundamentals must be organized and financed by the subject of the Federation. This corresponds to the principle of delineation of powers between federal government bodies, government bodies of the constituent entities of the Russian Federation and local government bodies, however, it will create difficulties in practical health care in the organization and financing of specialized medical care in municipal health care organizations.
Art. 41 is devoted to medical and social assistance to citizens suffering from socially significant diseases. In accordance with the new Fundamentals, measures of social support in the provision of medical and social assistance and drug provision to these citizens are established not at the federal level, but by the state authorities of the constituent entities of the Russian Federation. Financial support of measures to provide medical and social assistance to these citizens is an expenditure obligation of the constituent entities of the Russian Federation.
The question involuntarily arises: are there socially significant diseases in a particular region, and the state as a whole is not responsible for diseases that have arisen for social reasons? In addition, with different financial capabilities of the constituent entities of the Federation, a patient with the same disease will have different opportunities when receiving medical and social assistance in different territories.
Art. 42 is devoted to medical and social assistance to citizens suffering from diseases that pose a danger to others. In accordance with the new Fundamentals, the word "free" has been removed when providing medical and social assistance to these citizens. Medical and social assistance to citizens suffering from diseases that pose a danger to others, in accordance with the amendments, is provided only in institutions of the state health care system intended for this purpose (municipal health organizations are excluded) within the framework of the Program of state guarantees for the provision of free medical care to citizens of the Russian Federation. Measures of social support in the provision of medical and social assistance and drug provision to these citizens are established not at the federal level, but by the state authorities of the constituent entities of the Russian Federation. Financial provision of measures for the provision of medical and social assistance to citizens suffering from diseases that pose a danger to others is an expenditure obligation of the constituent entities of the Russian Federation.
In addition, medical and social assistance to citizens suffering from diseases that pose a danger to others cannot be provided only within the framework of the Program of state guarantees for the provision of free medical care to citizens of the Russian Federation, because the territorial programs developed in accordance with the federal program do not take into account the types and the volume of medical care in the context of epidemics and, accordingly, are not funded for this case.
In connection with the changed social policy, Art. 50. Medical and social expertise. This article is presented in the following edition.
Medical and social expertise is carried out by federal institutions of medical and social expertise in the manner prescribed by the legislation of the Russian Federation.
A citizen or his legal representative has the right to invite, at his request, any specialist with his consent to participate in the medical and social examination.
Section X. Rights and social support of medical and pharmaceutical workers.
In Art. 56. The right to engage in private medical practice - the part defining the powers of the local administration to issue a permit to engage in private medical practice in the jurisdictional territory has been declared invalid. Private medical practice is carried out on the basis of a license; the establishment of the procedure for licensing medical activities falls under the authority of federal government bodies.
Control over the quality of medical care is carried out by the federal executive body, whose competence includes the implementation of state control and supervision in the field of health care, unless otherwise provided by federal law.
Thus, legislatively strengthened control over the activities of the private health care system by the federal executive body. The question arises of how the Ministry of Health and Social Development of the Russian Federation will be able to organizationally carry out this control in all regions of the vast country.
Art. 59. General practitioner (family doctor) - stated as follows.
General practitioner (family doctor) - a doctor who has undergone special multidisciplinary training in the provision of primary health care to family members, regardless of their gender and age.
The procedure for carrying out the activities of a general practitioner (family doctor) is established by the federal executive body in the field of health care, executive bodies of the constituent entities of the Russian Federation.
Significant changes have been made to Art. 63. Social support and legal protection of medical and pharmaceutical workers.
The right to priority receipt of residential premises, the installation of a telephone, the provision of places for their children in preschool and sanatorium-resort institutions, the purchase on preferential terms of vehicles used to perform professional duties with a traveling nature of work, and other benefits provided by law are excluded. The right of doctors, pharmacists, workers with secondary medical and pharmaceutical education of the state and municipal health care systems, working and living in rural areas and urban-type settlements, as well as their family members living with them, to the free provision of apartments with heating and lighting in accordance with the current legislation is excluded. legislation.
These rights, despite their legislative consolidation, were not implemented.
In this case, there is a clear tendency to build a legal state based on the rule of law. In the laws adopted during the period of socialism and post-socialism, they did not skimp on rights, but some of the rights did not have mechanisms for implementation. This did not seem so important, since there was no obligation to enforce the laws. State administrative mechanisms worked both to protect the citizen and to suppress him. With the establishment of the rule of law, the role of law in society has increased, citizens have learned to defend their rights in court, enshrined in the law. Taking this into account, the modern legislator follows the path of limiting rights and compliance of legislation with the existing state of affairs, i.e., the possibilities of exercising the right.
This article is supplemented by the following parts.
Measures of social support for medical and pharmaceutical workers of federal specialized health organizations are established by the Government of the Russian Federation.
Measures of social support for medical and pharmaceutical workers of healthcare organizations under the jurisdiction of the constituent entities of the Russian Federation are established by the state authorities of the constituent entities of the Russian Federation.
Measures of social support for medical and pharmaceutical workers of municipal health organizations are established by local governments.
This corresponds to the principle of differentiation of powers between federal government bodies, government bodies of the constituent entities of the Russian Federation and local government bodies, however, the division of medical workers in matters of social support by levels - federal, regional and municipal - will lead to inequality of citizens' rights on the territory of the state.
Art. 64. Compulsory insurance of medical, pharmaceutical and other employees of the state and municipal health care systems whose work is associated with a threat to their life and health is set out in the following edition.
For medical, pharmaceutical and other employees of the state and municipal health care systems, whose work is associated with a threat to their life and health, compulsory insurance is established in accordance with the list of positions, the occupation of which is associated with a threat to the life and health of employees, approved by the Government of the Russian Federation.
The amount and procedure for compulsory insurance for medical, pharmaceutical and other employees of federal specialized healthcare organizations whose work is associated with a threat to their life and health are established by the Government of the Russian Federation. The amount and procedure for compulsory insurance for medical, pharmaceutical and other health care workers under the jurisdiction of the constituent entity of the Russian Federation, whose work is associated with a threat to their life and health, are established by the state authorities of the constituent entity of the Russian Federation.
The amount and procedure for compulsory insurance for medical, pharmaceutical and other employees of municipal health organizations, whose work is associated with a threat to their life and health, are established by local government bodies.
In the event of the death of employees of the state and municipal health care systems in the performance of their labor duties or professional duty during the provision of medical care or scientific research, the families of the victims are paid a one-time cash allowance.
The amount of a one-time cash benefit in the event of the death of employees of federal specialized healthcare organizations is established by the Government of the Russian Federation.
The amount of a one-time cash allowance in the event of the death of employees of health care organizations under the jurisdiction of a constituent entity of the Russian Federation is established by the state authorities of the constituent entity of the Russian Federation.
The amount of a one-time cash benefit in the event of the death of employees of municipal health organizations is established by local government bodies.
In accordance with Art. 15 of the new law amended the Law of the Russian Federation dated 02.07.92 No. 3185-1 "On psychiatric care and guarantees of citizens' rights during its provision".
In Art. 16 the organization of the provision of psychiatric care is entrusted to federal specialized medical institutions, the list of which is approved by the Government of the Russian Federation, and specialized medical institutions of the constituent entities of the Russian Federation. Thus, local governments are not involved in providing the population with psychiatric care.
The solution of issues of social support and social services for persons suffering from mental disorders in difficult life situations is carried out by the state authorities of the constituent entities of the Russian Federation.
Art. 17. Financing of mental health care - set out as follows.
Financial support of psychiatric care provided to the population in federal specialized medical institutions, the list of which is approved by the Government of the Russian Federation, is an expenditure obligation of the Russian Federation.
Financial support for the provision of psychiatric care to the population (with the exception of psychiatric care provided in federal specialized medical institutions, the list of which is approved by the Government of the Russian Federation), as well as social support and social services for persons suffering from mental disorders in difficult life situations, is an expenditure obligation of the subjects Russian Federation.
With a lack of financial resources, the constituent entities of the Federation are unlikely to be interested in the development of a psychiatric service, this category of patients in a number of regions may find themselves without specialized medical care.
Art. 22. The guarantees for psychiatrists, other specialists, medical and other personnel involved in the provision of psychiatric care are set out in the following edition.
1) Psychiatrists, other specialists, medical and other personnel involved in the provision of psychiatric care have the right to a shorter working time, additional leave for work in especially hazardous to health and difficult working conditions in accordance with the legislation of the Russian Federation.
2) Psychiatrists, other specialists, medical and other personnel involved in the provision of psychiatric care are subject to compulsory insurance in the event of harm to their health or death while on duty in the manner prescribed by the legislation of the Russian Federation; compulsory social insurance against industrial accidents and occupational diseases in the manner prescribed by the legislation of the Russian Federation.
The question arises, what is the difference between working with patients with mental illness in federal healthcare institutions from working with patients with mental illness in medical institutions of the constituent entities of the Russian Federation, if the personnel working with them will have different allowances?
In Art. 45, the procedure for monitoring mental health care activities has been changed. Control over the activities of federal psychiatric and neuropsychiatric institutions is carried out by authorized federal executive bodies, control over the activities of psychiatric and neuropsychiatric institutions under the jurisdiction of a constituent entity of the Russian Federation is exercised by the authorized federal executive body and executive bodies of the constituent entities of the Russian Federation.
Control over the activities of federal psychiatric and neuropsychiatric institutions is carried out in the manner determined by the Government of the Russian Federation.
In accordance with Art. 32 of the new law amended the Law of the Russian Federation dated 09.06.93 No. 5142-1 "On the donation of blood and its components".
In Art. 1 removed the upper age limit. A donor of blood and its components can be any capable citizen aged 18 years (in the old edition - up to 60 years) who has undergone a medical examination.
The article on federal programs for the development of blood donation has been excluded. There will no longer be such programs that are legally binding on the state.
Art. 4. Provision of measures for the development, organization and promotion of donation of blood and its components - set out in the following edition.
Financial support of measures for the development, organization and promotion of donation of blood and its components, carried out in order to ensure specialized medical care provided by federal health organizations, is an expenditure obligation of the Russian Federation.
Financial support of measures for the development, organization and promotion of the donation of blood and its components, carried out in order to provide specialized medical care (with the exception of that provided by federal health organizations), specialized (sanitary and aviation) emergency medical care, is an expenditure obligation of the constituent entities of the Russian Federation.
Financial provision of measures for the development, organization and promotion of the donation of blood and its components, carried out in order to ensure the provision of primary health care, medical care to women during pregnancy, during and after childbirth and emergency medical care (except for air ambulance), is an expenditure obligation of municipalities.
The implementation of measures for the development, organization and promotion of the donation of blood and its components is carried out on the basis of the creation of a unified information base in the manner established by the Government of the Russian Federation.
Art. 11 defines measures of social support for persons awarded with the "Honorary Donor of Russia" badge. Financial support of expenses related to the implementation of the rights of honorary donors remains an expenditure obligation of the Russian Federation, that is, with great difficulty, but it was possible to defend the financing of social support measures for honorary donors from the federal budget.
In accordance with Art. 48 of the new law, amendments have been made to the Federal Law of March 30, 1995 No. 38-FZ "On the prevention of the spread in the Russian Federation of a disease caused by the human immunodeficiency virus (HIV)."
In Art. 4. State guarantees - the following changes have been made.
The state guarantees the provision of medical care to HIV-infected - citizens of the Russian Federation in accordance with the Program of state guarantees for the provision of free medical care to citizens of the Russian Federation, as well as the provision of free medicines for the treatment of HIV infection on an outpatient basis in federal specialized medical institutions in accordance with the procedure established by the Government of the Russian Federation. Federation, and in health care institutions under the jurisdiction of the constituent entity of the Russian Federation, in the manner prescribed by the state authorities of the constituent entities of the Russian Federation.
Art. 6. Financial support of activities to prevent the spread of HIV infection - set out in the following version.
Financial support of measures to prevent the spread of HIV infection, carried out by federal specialized medical institutions and other organizations of federal subordination, refers to the expenditure obligations of the Russian Federation.
Financial support of measures to prevent the spread of HIV infection, carried out by health care institutions under the jurisdiction of the constituent entities of the Russian Federation, refers to the expenditure obligations of the constituent entities of the Russian Federation.
Art. 21. State lump sum benefits, invalidated. Thus, the right of employees of enterprises, institutions and healthcare organizations, whose work is related to the diagnosis, treatment of HIV-infected patients and materials containing HIV, to receive state lump-sum benefits in case of HIV infection in the line of duty has been eliminated.
Art. 22. Labor guarantees - set out in the following edition.
1. Employees of enterprises, institutions and organizations of the state health care system carrying out diagnostics and treatment of HIV-infected people, as well as persons whose work is related to materials containing the human immunodeficiency virus, have the right to reduced working hours, additional leave for work in especially dangerous for health and difficult working conditions in accordance with the legislation of the Russian Federation.
The procedure for providing these guarantees and establishing the amount of bonuses to official salaries for work in especially hazardous to health and difficult working conditions for employees of federal healthcare institutions is determined by the Government of the Russian Federation.
The procedure for the provision of these guarantees and the establishment of the amount of bonuses to official salaries for work in especially hazardous to health and difficult working conditions for employees of healthcare institutions of the constituent entities of the Russian Federation is determined by the executive authorities of the constituent entities of the Russian Federation.
2. Employees of enterprises, institutions and organizations of the state health care system carrying out diagnostics and treatment of HIV-infected, as well as persons whose work is related to materials containing the human immunodeficiency virus, are subject to compulsory insurance in case of harm to their health or death while on duty. in the manner prescribed by the legislation of the Russian Federation; compulsory social insurance against industrial accidents and occupational diseases in the manner prescribed by the legislation of the Russian Federation.
The same question arises: what is the difference between working with HIV-infected blood in federal healthcare institutions from working with HIV-infected blood in medical institutions of the constituent entities of the Russian Federation, if the personnel have different allowances?
In accordance with Art. 135 of the new law amended the Federal Law of 18.06.01 No. 77-FZ "On the Prevention of the Spread of Tuberculosis in the Russian Federation".
In Chapter II, the powers of local self-government bodies are removed from the powers in the field of preventing the spread of tuberculosis, thus all powers in this area are distributed between the Russian Federation and the constituent entities of the Russian Federation.
The powers of the Russian Federation to ensure economic, social and legal conditions to prevent the spread of tuberculosis have been removed from the powers of the Russian Federation.
Art. 5. The powers of the constituent entities of the Russian Federation in the field of preventing the spread of tuberculosis are set out as follows.
The constituent entities of the Russian Federation shall organize the prevention of the spread of tuberculosis, including anti-tuberculosis care for patients with tuberculosis in anti-tuberculosis dispensaries, other specialized medical anti-tuberculosis organizations and other healthcare institutions of the constituent entities of the Russian Federation.
It is known that tuberculosis is a socially significant disease, and only the state as a whole can solve the problem of socially significant diseases, influencing the economic, social and legal living conditions of people,
The refusal of the state to influence the social conditions of people's life, the redistribution of responsibility for measures of social support and financial support of measures for the provision of medical and social assistance to citizens suffering from socially significant diseases to the state authorities of the constituent entities of the Russian Federation will lead to a worsening of the situation with these diseases. And the point is not only that the subjects do not have enough money in the budgets to treat such a pathology. A separate constituent entity of the Federation, no matter how good everything is in this constituent entity (even an oil-producing, rich region that is a donor of the federal budget, capable of providing social support to the inhabitants of its region), cannot influence the situation in the country as a whole. No one can limit the constitutional right of a citizen to free movement, choice of place of stay and residence (Article 27 of the Constitution of the Russian Federation), therefore, patients with socially significant diseases can move to regions with a more funded system of social support. The influx of socially disadvantaged citizens into the regions, namely, they most often have socially significant diseases, is unlikely to have a positive effect on the development of these regions.
In addition, the decrease in the responsibility of the state for the social processes taking place in this state is a blow to the authority of the state as a whole, undermines faith in the social orientation of state policy.
The provision of anti-tuberculosis care to citizens in accordance with the adopted amendments is carried out not on the basis of the principle of gratuitousness (in the old edition), but in the volumes envisaged by the Program of state guarantees for the provision of free medical care to citizens of the Russian Federation. The program of state guarantees for the provision of free medical care to citizens of the Russian Federation is implemented in the territories through territorial programs that are funded in different territories in different ways. Thus, with insufficient financing of the territorial program of state guarantees for the provision of free medical care to citizens of a particular constituent entity of the Russian Federation, there may be restrictions on the required volume of medical care for patients with tuberculosis. This will lead to a worsening of the already unfavorable epidemic situation for tuberculosis in certain regions and in the country as a whole.
The exclusion from the rights of persons under observation in connection with tuberculosis and tuberculosis patients of the right to free travel on public transport in urban and suburban traffic when they call or refer to consultations in medical anti-tuberculosis organizations is unlikely to contribute to an improvement in the epidemic situation, especially in rural areas ...
The rights of persons under surveillance for tuberculosis and patients with tuberculosis to be provided with free medicines for the treatment of tuberculosis are set out as follows.
Persons under dispensary supervision in connection with tuberculosis and patients with tuberculosis are provided with free medicines for the treatment of tuberculosis on an outpatient basis in federal specialized medical institutions in accordance with the procedure established by the Government of the Russian Federation, and in health care institutions under the jurisdiction of the constituent entities of the Russian Federation - in the procedure established by the state authorities of the constituent entities of the Russian Federation.
Patients with infectious forms of tuberculosis living in apartments in which, based on the occupied living space and the composition of the family, it is impossible to allocate a separate room for a patient with an infectious form of tuberculosis, communal apartments, dormitories, as well as families with a child sick with an infectious form of tuberculosis, are provided outside queues of individual living quarters, taking into account their right to additional living space in accordance with the legislation of the constituent entities of the Russian Federation.
Art. 15. Social support of medical, veterinary and other workers directly involved in the provision of anti-tuberculosis care - set out in the following edition.
1. Medical, veterinary and other workers directly involved in the provision of anti-tuberculosis care, as well as employees of organizations for the production and storage of livestock products serving farm animals with tuberculosis, have the right to a reduced working time, additional leave for work in especially hazardous to health and difficult working conditions in accordance with the legislation of the Russian Federation.
The procedure for providing these guarantees and establishing the amount of bonuses to official salaries for work in especially hazardous to health and difficult working conditions for employees of federal healthcare institutions is determined by the Government of the Russian Federation.
The procedure for the provision of these guarantees and the establishment of the amount of bonuses to official salaries for work in especially hazardous to health and difficult working conditions for employees of healthcare institutions of the constituent entities of the Russian Federation is determined by the executive authorities of the constituent entities of the Russian Federation.
2. Medical, veterinary and other workers directly involved in the provision of anti-tuberculosis care, as well as employees of organizations for the production and storage of livestock products serving farm animals with tuberculosis, are subject to compulsory insurance in case of harm to their health or death in the performance of official duties in accordance with established by the legislation of the Russian Federation; compulsory social insurance against industrial accidents and occupational diseases in the manner prescribed by the legislation of the Russian Federation.
The same question: what is the difference between working with tuberculosis in federal healthcare institutions from working with tuberculosis in medical institutions of the constituent entities of the Russian Federation?
These are the main changes made to the Russian healthcare legislation in connection with the adoption of the new law. Also, serious changes have been made to federal laws in the field of public health, directly related to the legislation on health care: "On the immunization of infectious diseases" (dated 17.09.98 No. 157-FZ); "On the sanitary and epidemiological well-being of the population" (dated March 30, 1999, No. 52-FZ); "On Medicines" (dated 22.06.98 No. 86-FZ); "On the quality and safety of food products" (dated 02.01.2000 No. 29-FZ); "On Specially Protected Natural Areas" (dated 14.03.95 No. 33-FZ).
In general, it should be noted that although the delineation of powers between federal government bodies, government bodies of the constituent entities of the Russian Federation and local government bodies, of course, had the goal of changing the system of interbudgetary financial relations within the Federation, including health financing, the law did not simplify, but complicated the organization and inter-budgetary relations for the financial provision of medical care. For example, there will be difficulties with the realization of the right of citizens to medical care in the provision of emergency, primary health care, specialized medical care due to the lack of funds in the relevant budgets. Ensuring state guarantees of the right of citizens to health care and medical care (Article 41 of the Constitution of the Russian Federation) will still require the allocation of subventions to regional and local budgets in the amount necessary for the implementation of territorial programs of state guarantees for the provision of free medical care to citizens for the main types and volumes of medical care stipulated in the federal program.
2.2 Topical issues of legal regulation of the economic aspects of the activities of health care institutions
In modern conditions, not only the medical, but also the economic side of the activities of healthcare institutions is largely determined by the current regulatory framework.
The transformation of medical institutions from ordinary consumers of budgetary resources into independent economic entities, the introduction of compulsory and voluntary health insurance, the development of entrepreneurial activity and other innovations required a significant reform of the methods of economic activity. Meanwhile, there are serious problems in the legal regulation of the economic aspects of the activity of medical institutions, which can be grouped as follows: the lack of legal regulation of certain aspects of the activity of medical institutions; insufficient legal framework in certain areas of activity; contradictory legal regulation; the existence of legal norms that have a controversial interpretation; inconsistency of legal regulation with the tasks of health care development or the interests of the state; insufficient legal literacy of heads of medical institutions; problems of implementation of the legal rights of medical institutions in economic matters.
Let's consider these groups of problems in more detail.
Lack of legal regulation of certain aspects of the activities of medical institutions. The dynamism of the processes taking place in society and, in particular, in health care, leads to the fact that legal regulation does not keep pace with the pace of reforms. Therefore, at present, there is no legal regulation of a number of economic issues of the activities of health care institutions. This applies, for example, to some aspects of the activities of medical institutions related to the use of state (municipal) property in the implementation of entrepreneurial activities by budgetary medical institutions. In particular, this applies to the use of buildings (premises). Budgetary medical institutions within the framework of their main activity use buildings and structures free of charge. Accordingly, there is no methodological or regulatory framework for including the cost of these resources (depreciation) in the prices for paid services. However, prices for paid services are guided by the market level, which is formed primarily by commercial non-state medical institutions and includes all types of costs, including depreciation of buildings. In this situation, budgetary institutions, providing paid services at market prices, receive excess profits, the real basis of which is the unreimbursed cost of buildings (in the form of depreciation or rent).
Currently, there is no necessary legal regulation and a number of issues related to guarantees for the provision of free medical care. Everyone is well aware that the types and volumes of medical care envisaged by the programs of state guarantees for providing citizens with free medical care exceed the financial capabilities of the budget and the funds of compulsory medical insurance (MHI). It is no coincidence that even in the Address of the President of the Russian Federation to the Federal Assembly of the Russian Federation in 2001, it was noted that "... in the vast majority of regions this program is not provided with state funds. The deficit of funds under this program is 30-40 percent of the need, and it is covered .. . the forced expenses of patients to pay for drugs and medical services. " Meanwhile, medical institutions cannot fail to fulfill the program of state guarantees, and there is no officially established mechanism for compensating for the lack of financial support for the territorial program of state guarantees at the expense of the budget or funds of the population. There is also no normative regulation of the situation of exceeding within the framework of a particular medical institution or the entire territory of the volume of free assistance provided for by the program. It is quite clear that an institution (doctor) cannot refuse to provide medical care to a patient on the grounds that the institution has already exceeded the planned volumes approved by the program. This would be in violation of a number of laws, including the Criminal Code. But can the institution (at least theoretically) offer the population to pay for medical services provided in excess of the scope of the program? Neither the decree of the Government of the Russian Federation of 11.09.98 No. 1096 "On the approval of the program of state guarantees for providing citizens of the Russian Federation with free medical care", nor other normative acts devoted to this problem, give an answer to this question.
Meanwhile, in many countries (for example, in Kyrgyzstan) various forms of partial participation of the population in financing the provision of medical care are used. These are the so-called copayments. There is currently no legal regulation of this form of compensation for the lack of budgetary funding or compulsory medical insurance funds.
Lack of legal framework in certain areas of activity. Ten years of experience in the work of medical institutions in the compulsory medical insurance system revealed the need to improve legislation in this area. Let's give an example. The current legislation does not provide a clear definition of what level of budget funds should be used to carry out compulsory medical insurance (who exactly should be the insured) of the non-working population. In Art. 2 of the Law "On Medical Insurance of Citizens in the Russian Federation" states that the number of insurers of the non-working population includes both the state authorities of the constituent entities of the Federation and the local administration. Therefore, in different regions this problem is solved in different ways: in some regions, insurance of the non-working population is carried out at the expense of the budget of the subject of the Federation, in others - at the expense of municipal (district) budgets. This and many other problems are intended to be resolved by the law "On Compulsory Health Insurance", which is being drafted now.
The legal regulation of relations in the field of private medical activity cannot be considered sufficient either. Medical activity is a special type of activity with a high risk to life and health. In the private health sector, in contrast to the state and municipal, there are no governing bodies and structures that organize this activity, exercise leadership and control. In order to fill these gaps, the State Duma Health and Sports Committee has prepared a draft federal law "On the regulation of private medical activity."
The increase in the volume of paid services provided by state and municipal medical institutions also revealed a number of problems related to the procedure for their provision. In some cases, there is an uncontrolled development of the entrepreneurial activity of medical institutions, which is detrimental to the interests of the state and the population, in other cases, higher authorities put obstacles to reasonable directions for the provision of paid services. This is caused primarily by the weak development of the regulatory framework for the provision of paid services in healthcare. At the same time, there is a fairly clear legal basis for the entrepreneurial activity of non-profit organizations (which include budgetary medical institutions), taxation, etc., fixed in a number of adopted laws, decrees of the Government of the Russian Federation and other regulatory legal acts. Therefore, the insufficient development of the regulatory framework is manifested mainly in the absence of a clear mechanism for regulating the procedure for the provision of paid medical services, enshrined in the departmental regulations of the Ministry of Health of the Russian Federation (orders, instructions, etc.). Departmental regulations are intended to provide an interpretation of legislative and other legal acts in relation to medical institutions, taking into account the specifics of the industry. Meanwhile, even the main order of the Ministry of Health of the Russian Federation regulating the procedure for the provision of paid services (dated March 29, 1996, No. 109 "On the rules for the provision of paid medical services to the population"), only duplicated the Resolution of the Government of the Russian Federation of January 13, 1996 No. 27 "On approving the rules for the provision of paid medical services. to the population by medical institutions ", without introducing anything new. It is quite obvious that these rules do not cover the entire list of issues that arise in the provision of paid services. Not filling all the gaps and other few orders of the Ministry of Health of the Russian Federation, affecting the provision of paid services (dated 20.03.92 No. 93 "An indicative list of medical services provided at the expense of state, public organizations, institutions, enterprises and other economic entities with any form of ownership, as well as personal funds of citizens "; dated 06.08.96 No. 312" On the organization of the work of dental institutions in the new economic conditions of management ", etc.).
An example of the inconsistency of legal regulation is the situation with the taxation of the activities of health care institutions in the CHI system. As you know, state extra-budgetary funds (which include the CHI fund) are included in the budgetary system of the Russian Federation (Article 6 of the Budget Code of the Russian Federation). Therefore, in accordance with Art. 251 of the Tax Code of the Russian Federation, the amounts of financing from the budgets of state extra-budgetary funds refer to earmarked receipts, that is, to incomes that are not taken into account when determining the tax base of income tax. However, in practice, medical institutions usually receive these funds not directly from CHI funds in the form of direct financing, but through medical insurance organizations under civil law contracts in accordance with the volume of services provided. In many cases, the tax authorities refuse to recognize these revenues as earmarked receipts and insist on including them in the tax base.
Unfortunately, in many respects, changes in tax legislation also have an adverse effect on the filling of regional and local budgets and, accordingly, on the financial possibilities of supporting health care. Thus, as a result of tax changes, the regions in recent years have lost a significant part of the revenues that went to the federal budget. At the same time, the main financial burden for providing citizens with free medical care remains with the regions - local budgets and the budgets of the constituent entities of the Federation. Moreover, the state policy aimed at easing the tax burden, while positive in itself, in many cases turns out to be unprofitable for regional budgets (and, accordingly, for health care). For example, according to the current legislation, the bulk of the profit tax is directed to the budgets of the constituent entities of the Federation, and the decrease in the tax rate of the profit tax has the greatest effect on the regional budgets. As for the positive aspects of reducing the tax burden, they are manifested primarily in stimulating production growth, the logical result of which is an increase in tax revenues from value added tax, which, in turn, is directed to the federal budget.
Serious contradictions in legal regulation are also revealed by the implementation of the RF law "On health insurance of citizens in the Russian Federation." The lack of legal regulation in the field of compulsory medical insurance has already been noted above. Here I would like to draw your attention to the presence of contradictions of the above law with other regulations. Despite the existence of a law establishing uniform principles of health insurance, each constituent entity of the Federation implements its own CHI models, and often directly contradicting the principles laid down in the law (there are no insurance organizations or territorial CHI funds; executive authorities do not contribute funds for insurance of the unemployed population, etc.) etc.). This was the result of both the imperfection of the law itself, which is mostly declarative in nature, and the fact that it came into conflict with a number of legislative acts granting broad rights to the subjects of the Federation in regulating financial and social issues in their regions.
The presence of legal norms with a controversial interpretation. Among the legal norms that cause the greatest number of disputes on economic issues are the issues of remuneration and pricing in the provision of paid services by medical institutions. Thus, the current Labor Code of the Russian Federation (Article 135) determines that the establishment of wages for employees of organizations with mixed financing (budgetary financing and income from entrepreneurial activities) is carried out in accordance with laws, other regulatory legal acts, collective agreements, agreements, local regulations organizations. Higher-level healthcare authorities usually interpret this article as follows: collective agreements, agreements, local regulations of medical institutions are valid if they do not contradict the current regulations and decisions of higher authorities (including orders of the relevant healthcare authority). Formally, this is the correct interpretation, but it does not take into account differences in funding sources. The fact is that, as can be seen from the previous phrase of the same article of the Labor Code, by the relevant laws and other regulatory legal acts, wages are established only for employees whose activities are financed from the budget. It follows from this that for workers who provide paid services, wages are established by collective agreements, agreements, local regulations of organizations, that is, medical institutions independently regulate this issue, especially since in Art. 161 of the Budget Code of the Russian Federation states that "a budgetary institution, when executing estimates of income and expenses, independently in spending funds received from extra-budgetary sources."
Another issue that has a different interpretation is the application of a state (municipal) contract (order) to the services of budgetary medical institutions. As you know, a state or municipal contract can be concluded by a public authority or a local self-government body, a budgetary institution, an authorized body with individuals and legal entities in order to meet state or municipal needs. However, practice shows that the concept of a state (municipal) contract or order is practically not used for the procurement of medical services from the budgetary healthcare institutions themselves, although this is quite consistent with the concept of a contract (order) given in Art. 72 of the Budget Code. Considering that state and municipal contracts should be placed on a competitive basis, this would largely contribute to solving the urgent problem of restructuring the network of medical institutions.
The issue of borrowing by state and municipal budgetary health care institutions from third parties is also controversial. In Art. 118 of the Budget Code of the Russian Federation states that budgetary institutions are not allowed to receive loans from credit institutions and other individuals and legal entities, with the exception of loans from budgets and state extra-budgetary funds. The requirement seems to be logical: after all, in accordance with Art. 120 of the Civil Code of the Russian Federation, if the medical institution is unable to repay the loan, the owner of the corresponding property shall bear subsidiary responsibility for its obligations. However, medical institutions are expanding their business activities, which is difficult to do without the use of borrowed funds. Meanwhile, it is not entirely clear whether the restriction on borrowing, introduced by the Budget Code, applies only to the budgetary activities of state (municipal) medical institutions, or applies to extrabudgetary activities.
Inconsistency of legal regulation with the tasks of health care development or the interests of the state. In Art. 256 of the Tax Code of the Russian Federation states that property of budgetary organizations is not subject to depreciation, with the exception of property acquired in connection with entrepreneurial activities and used for such activities. This means that if a budgetary medical institution provides paid services using property acquired from the budget or from the compulsory medical insurance funds (and this is a widespread practice), then it cannot attribute the depreciation of this property to costs. As a result, state (municipal) property will be used to provide paid services free of charge. This situation could be considered as a kind of subsidization of the provision of paid services to the population, if not for 2 circumstances. First, these subsidies will also apply to those types of services that, by definition, should be provided only for a fee (service, cosmetology without medical indications, etc.). Secondly, such subsidies destabilize the market for paid (commercial) medical services, since private institutions are deprived of this subsidy and are forced to provide services at a full, higher price. All this leads to the well-known costs associated with the disruption of normal market processes. In our opinion, the problem should be solved in a different way: it is necessary to include in the price of a paid service of depreciation of any used property, but that part of depreciation that is charged on state (municipal) property should be returned to the budget or taken into account as part of budget financing.
The legal regulation of voluntary health insurance does not always meet the interests of society. For example, in Art. 1 of the RF Law "On Medical Insurance of Citizens in the Russian Federation" states that "voluntary medical insurance is carried out on the basis of voluntary medical insurance programs and provides citizens with additional medical and other services in excess of those established by compulsory medical insurance programs." From the content of this article it follows that the voluntary medical insurance program for employees of a highly profitable enterprise, bank, etc. the types of assistance included in the territorial compulsory medical insurance program cannot be present. It turns out that wealthy enterprises or citizens are ready to fully pay for medical care at their own expense, without resorting to compulsory medical insurance services (thereby saving compulsory medical insurance funds to provide free assistance to less wealthy citizens), and the law limits them in this desire. Obviously, an increase in the number of grounds is required to expand the scope of the voluntary health insurance program (for example, if the insured wish, etc.).
In our opinion, many provisions of the legislation in the field of taxation do not meet the objectives of health care development. In particular, this concerns the introduction of a value added tax on medicines, the spread of sales tax to paid medical services, and the very procedure for taxing the income of medical institutions from the provision of paid services. All this reduces the already meager financial potential of health care, reduces the availability of paid services and medicines for the population.
Insufficient legal literacy of heads of medical institutions. Unfortunately, we have to admit that the legal literacy of the heads of medical institutions leaves much to be desired. Meanwhile, knowledge of the basic regulatory documents and general legal principles relating to the activities of a medical institution allows not only to carry out their activities more efficiently, but also in many cases to defend their legal rights. In addition to improving the legal training of medical students and students of advanced training courses, it is necessary to introduce legal advisers to the staff of all medical institutions or conclude contracts for legal services for the activities of medical institutions.
Problems of the implementation of the legal rights of medical institutions in economic matters. Unfortunately, knowledge of legislation is far from sufficient to use it in practice. Medical institutions very often have to deal with situations when they clearly understand the legal side of the problem, but cannot act in accordance with the existing legislation. In particular, this concerns the issues of pricing for paid medical services. In accordance with the decree of the Government of the Russian Federation dated 07.03.95 No. 239 "On measures to streamline state regulation of prices (tariffs)", state regulation of prices for paid medical services is not provided. In order to clarify this issue, in the letter of the Ministry of Economy of the Russian Federation dated 03.03.99 No. 7-225 "On prices for paid medical services" it was reported that state regulation of prices (tariffs) does not apply to paid services, the list of which is not provided for by the decree of the Government of the Russian Federation dated 07.03.95 No. 239. Nevertheless, almost everywhere government or health authorities intervene in pricing issues.
Other issues on which medical institutions often experience unreasonable pressure from higher authorities include the level of wages included in the prices of paid services; use of income received from entrepreneurial activity; remuneration of employees at the expense of income received from the provision of paid services, etc.
Of course, medical institutions can resort to such a form of protection of their legal rights as going to court. However, practice shows that medical institutions rarely use this right, because, having won a lawsuit, the head of the institution may lose his position. The higher authorities have plenty of opportunities for this. The legal insecurity of the head of a medical institution is another serious problem that limits the scope of the legal field in healthcare.
In conclusion, we note that we have touched on only a small part of the issues related to the regulatory framework for reforming the health care economy, but the issues considered indicate the presence of serious problems in this area. It is obvious that the improvement of the legal regulation of the economic aspects of the activities of medical institutions should not only be based on the fundamental principles of law, requirements for the protection of the rights and freedoms of citizens, respect for the interests of the state, etc., but also comply with economic laws, contribute to the effective economic activity of health care institutions.
In order to improve the legal framework for health protection, including the solution of many economic issues, the Committee for Health Protection and Sports of the State Duma
carries out a lot of work to improve legislation in the field of healthcare. It is expressed not only in the introduction of amendments to existing laws and the development of new bills, but also in the systematic formation of the Code of Laws on the Protection of Public Health.
At the same time, it is obvious that most of the problems discussed above cannot be solved only within the framework of legislation in the field of health care, since changes (amendments) are required in a number of legislative acts of a more general plan (Civil, Budget, Tax Codes, etc.). In addition, executive authorities (the Government of the Russian Federation, the Ministry of Health of the Russian Federation, etc.), as well as the legislative bodies of the constituent entities of the Federation, should play a large role in improving the legal regulation of the economic sphere of health care.
3. Problems of public administration in the field of health care and ways to solve them
3.1 Problems of improving the organization of medical care for the population
The organization of medical care in rural areas has a number of features, among which a small number of the served population living in a fairly large territory can be distinguished; the predominance of non-working and pensioners among rural residents; the lack of opportunities for the population of the rural area to fully exercise the right to choose a medical institution.
The socio-economic transformations of recent decades have complicated the availability of medical care to the rural population, have not improved the quality and have not raised the level of its organization. Since the beginning of the 1990s, there has been a decrease in the resource provision of rural health care. Weak medical and diagnostic base, low material and technical equipment, low level of development of information technologies - this is not a complete list of the current state of rural medical institutions. Along with the aforementioned difficulties, one of the serious problems of practical health care in modern conditions is the low efficiency of using the resource base. The main task of improving the organization of medical care for the rural population is reasonably to reorient the main efforts from the hospital stage to the outpatient one, i.e., restructuring care while improving its quality and reducing costs. Analyzing the real changes that took place at the end of the last and the beginning of the new century, we can conclude that the reform processes, which have been sufficiently developed at the theoretical level and reflected in the Concept for the development of healthcare and medical science in the Russian Federation (1997), are proceeding slowly or almost absent in practice, and the structural effectiveness of the health care system as a whole remains lower than expected. It is necessary to increase interaction and continuity in the activities of all links of the system, the priority development of the outpatient-polyclinic link, the redistribution of the volume of activities and resource provision between the structures of hospital, community-based, medical and social care.
One of the main directions of improving the organization of medical care is the development of primary health care (PHC). A special role in this is assigned to the development of the institute of general (family) practice (GP). The World Health Organization, which regularly publishes rankings of health systems in countries of the world, considers the main thing not their scientific and material and technical base, but the availability of medical services for the population, which is largely determined by the state of primary health care. A doctor is needed who is able to take over all the first contacts with the population, promptly seek advice from more qualified, better equipped second-level specialists, and if necessary, send the patient to a hospital. The delay in establishing a GP service has a significant impact on the advancement of overall health care reform. The shift towards outpatient care and the reduction of unjustified volumes of medical care almost entirely depend on the development of the GP service, and this does not exclude the development of many hospital-substituting forms of medical care.
The main problems of organizing out-of-hospital care for the rural population according to the principle of general medical practice (GPP) are the imperfection of the regulatory and methodological framework governing the role and place of GPs in the rural health care system, the legal status of GPs, their interaction with other medical institutions, funding mechanisms for GPs; the lack of training standards for the staff of the GP that determine the list of knowledge and practical skills of the staff of the GP; the lack of developed standards for medical and technical support for AFP, which does not allow for their adequate equipping with medical equipment.
In the conditions of the transitional period from the service of district doctors to the GP, it is inappropriate to go by reducing the number of positions of doctors - narrow specialists. The experience of rural municipal health care facilities shows that there are not enough such doctors. Saving money on doctors - narrow specialists and reallocation of funds in favor of GPs at the moment will lead to a decrease in the availability of specialized free medical care to the population. Today, it is most profitable to introduce ORP in remote sparsely populated areas, in rural areas, as well as in economically favorable regions with a solvent population, for example, in Moscow, as a paid medical activity to serve certain categories of citizens.
Until now, in Western Europe, there is a high proportion of single practices (in the Netherlands - 54%, in the UK - 30%), which mainly operate in rural areas with a relatively low population density. In the UK, the GP visits patients at home less intensively than in Russia - in 15-20% of cases (visits to the elderly and people who cannot come to an appointment), and in Russia - in 30-40%, and a significant part of the visits in our country is not justified. Moreover, the reception of GPs in the UK and the Netherlands takes up to 8 minutes on average; a detailed conversation with the patient, in-depth diagnostic studies, detailed records in the outpatient card are not carried out.
The introduction of the GP institute in rural areas of the Chuvash Republic is accompanied by a significant economic effect. Already at the initial stage of implementation in the service area of these specialists, there is a decrease in the level of hospitalization by 5-10%, a decrease in the number of ambulance calls by 5-15%, and the number of referrals to narrow specialists has decreased by 10-15%.
One of the most cost-effective ways to provide medical services at the PHC level is nursing, which can be viewed as a savings reserve for regional and municipal health care. An AFP nurse, if properly trained, can be assigned many of the responsibilities that a physician performs today. This is how nursing staff operate successfully in European countries. The main forms of independent work of GP nurses are home patronage of the patient, conducting classes in "schools for patients", admission to the polyclinic. Medical care provided by a paramedic who has a certificate of a specialist in medical care is characterized by a large amount of medical and preventive work with sufficient quality of first-aid medical care. Important medical traditions are preserved - the provision of assistance by a paramedic at home to adults and children, including outside working hours. All this increases the role of the paramedic in the ORP system. The outpatient link can be significantly strengthened due to the reinforcement of paramedical personnel at the rate of a paramedic and two nurses for a population served from 2,800 to 3,200 people.
Until today, there has been no real reform of primary health care. The overwhelming majority of outpatient clinics continue to provide primary medical care by the local therapist and narrow specialists. Analysis of the implementation of the sectoral program "General medical (family) practice" showed the need to use a systematic approach in improving the regulatory, socio-economic, financial, material, technical, organizational, methodological and managerial mechanisms that determine the peculiarities of the organization and functioning of the GP service in the structure of the primary health care.
Within the framework of restructuring and improving the efficiency of healthcare, an important aspect is the development of hospital-substituting forms of medical care. So, at present, the proportion of daytime beds has reached 9% of the total bed capacity of municipal hospitals in the Moscow region. In rural areas, it is organizational and economically feasible to use hospital-replacing technologies in large and medium-sized settlements. The main goal of the development of such forms of organization of medical care is to reduce the rates of hospitalization in round-the-clock hospitals and, accordingly, to reduce the costs of the healthcare system while maintaining the quality of medical care and its availability.
Considering the system of organization of inpatient care for the rural population, a number of problems can be identified, including such as the low rate of completeness of prehospital examination; delays in hospitalizations, especially in regional health care facilities; a tendency towards an increase in the number of independent appeals of rural residents to city and regional, including specialized, hospitals; high and growing rate of emergency hospitalizations; a significant proportion of unjustified hospitalizations. The actual state of rural hospitals of the I and II levels (district and central regional hospitals) does not meet the requirements for either capacity, or material and technical equipment, or the composition and qualifications of personnel and specialization of the bed fund. In the district hospitals, a minimum amount of medical and diagnostic assistance is provided, patients are hospitalized in them who need not so much intensive therapy as medical and social assistance. Specialized inpatient care is increasingly shifting to regional and republican institutions. The problem of restructuring is being solved by transferring district hospitals to nursing homes, to the departments of rehabilitation treatment, rehabilitation and medical and social assistance, to medical outpatient clinics.
As part of the structural reorganization of inpatient medical care for the rural population, it is necessary to limit specialized care in the Central District Hospital (CRH), except for inter-district centers; close low-capacity (up to 25 beds) district hospitals or transfer them to the balance of social protection institutions; give priority to specialized inpatient care to regional hospitals and inter-district centers. In the CRH, the emphasis should be placed on general inpatient care (therapeutic, surgical, pediatric, obstetric and gynecological) with planned operations that do not require high-tech medical equipment.
The reduction of the bed capacity and the number of hospitalizations, meanwhile, is not an end in itself, it is a tool to optimize costs in the health care system. So, in order to reduce the number of unreasonable hospitalizations in a number of rural hospitals in the Samara region, diagnostic beds have been organized as part of the admission department for dynamic monitoring of patients who have no absolute indications for hospitalization. After carrying out medical and diagnostic procedures, only 33% of those admitted to the emergency department were hospitalized, which caused an economic effect. According to the standards, the financing schemes for outpatient and polyclinic institutions to pay for visits and hospitals on a completed case do not stimulate the chief doctors of hospitals to restructure the bed fund and expand the volume of out-of-hospital care. A hospitalization management system is proposed that allows to combine the prehospital and hospital stages into a single organizational and technical cycle, based on which the doctors of the district service strictly follow the algorithm for preparing patients for hospitalization. This is followed by an examination by the hospital by a specialist-manager for planned hospitalization, responsible for the level of prehospital examination, the validity of hospitalization, an even distribution of the flow of patients to the hospital by days of the week and time of day.
Taking into account the modest medical and diagnostic capabilities, the lack of qualified medical personnel, the weak material and technical base and the lack of financial resources of rural medical and preventive institutions, a special role is currently assigned to the development of specialized consultative medical care, in particular the development of mobile forms of medical diagnostic assistance, and especially creation of interdistrict consultative and diagnostic centers. To increase the real role of interdistrict centers, it is necessary to determine the correct forms of interaction and responsibility of the administrative bodies of municipalities included in the medical-sanitary zone; create an adequate financing system and an appropriate material and technical base; to ensure effective planning and control of the activities of inter-district centers as one of the levels of the system of providing specialized advice to the villagers. It is necessary to clearly define the areas served, taking into account the territorial location and transport accessibility, the number of the served population, the optimal distribution of types and volumes of care in the CRH system - the interdistrict center - the regional hospital, the organization and control of patient flows in the territorial medical-sanitary zone.
In rural areas, the problem of rational interaction between the social assistance system and health care is especially acute, given the larger proportion of elderly people living in rural areas. The literature data allow us to distinguish two main forms of medical and social services in rural areas: inpatient and out-of-hospital. The main types of inpatient institutions include medical and social departments based on rural hospitals, hospitals (departments, houses) of nursing care, hospices, as well as stationary institutions of social protection bodies (boarding houses, departments and houses of mercy, etc.). Outpatient forms of medical and social assistance to elderly rural residents include departments of outpatient medical and social assistance, outpatient services of social welfare agencies, and public organizations.
If in our country the medical and social direction in providing assistance to the elderly rural population began to actively develop from the early 1990s, then various forms of medical and social assistance began to appear abroad in the 1960s. Currently, medical and social assistance to elderly citizens in rural areas of developed foreign countries can be attributed to one of the main areas of medical care for the population, along with AFP. In European countries, out-of-hospital care for rural elderly people is mainly focused on home care with the wide involvement of social workers. According to researchers from Canada, in rural areas it is not worth organizing low-power day geriatric hospitals; it is advisable to have large inter-district centers where all the necessary specialists are concentrated. Despite the great variety of inpatient institutions of medical and social services noted abroad, the prevailing position in rural areas is occupied by nursing homes (departments), and to a lesser extent - by hospices. According to many authors, volunteers provide great assistance in the activities of these organizations.
Thus, according to the literature, there are a number of problems and directions in the optimization of medical care for the rural population. We must agree with the point of view that the reorganization of the structure of rural health care facilities, their resource provision allows for various forms of organization and the pace of transformations, but with the preservation of common approaches. We are talking here about the introduction of a general practitioner (paramedic); the deployment of specialized services based on the CRH; organization of interdistrict centers in large CRHs; bringing the bed capacity to the real needs of the population; organization of catering services for rural residents in various forms.
The mechanism for organizing medical care involves an analysis of the state of health of the population; assessment of the organization of medical care; analysis of health care management and financing systems of the constituent entities of the Federation and municipalities; setting strategic goals, objectives and priorities in the development of health care and the activities of health care facilities; determination of the real need for medical services based on expert assessments; optimization of the network and structure of institutions in the context of the implementation of the municipal order.
At present, the concept of integrating health care services at the district level is being developed abroad, and efforts are being combined in the process of information exchange, planning, improving infrastructure, developing human resources, and not only in relation to health authorities. Steps are being taken to develop and integrate health care, education, transport, communications, housing, water supply, small businesses, agriculture under the control of municipalities. Community participation in integrated services increases overall satisfaction with their work. Integration tends to smooth out differences between geographic areas and socioeconomic groups in terms of service availability and usage. A key factor in the process of integrating district health services is PHC, which should be comprehensive (include health promotion, prevention, control and rehabilitation), holistic (deal with the person as a whole in the context of the family and community), continuous (use a strategy of registering and registering regular follow-up of patients and monitoring of care).
In the current legislation on medical practice, there are not only significant shortcomings, but also gaps. Thus, the Constitution of the Russian Federation, designating health care systems, does not directly indicate the existence of a unified health care system in the Russian Federation, the constituent parts of which should be state, municipal and private health systems. Non-recognition of the constitutionality of the existence of a unified health care system means that in the absence of appropriate legal regulation, federal bodies, state authorities of the constituent entities of the Russian Federation, local self-government bodies do not have a direct constitutional obligation to preserve and develop the corresponding health care system on their territories as a whole.
At the same time, despite the absence of direct indications of this in the Constitution of the Russian Federation, the analysis of the relevant articles provides indirect grounds for considering the health care system in the Russian Federation as a constitutional institution, since the social character of the state is attributed by the Constitution to the foundations of the constitutional order. The content of constitutional norms establishes the need for a unified health care system that unites various forms of state, municipal and private health care subsystems in a specific territory. The need for a unified health care system in the Russian Federation is also indicated by the Concept for the Development of Health Care and Medical Science in the Russian Federation.
The obligation of the state to ensure social equality in the realization of the right to health protection for all citizens of the Russian Federation presupposes the presence of organizational unity and consistency in the prevention of diseases and their treatment. This goal can be effective only when creating a legislative framework aimed at creating a health care system in the Russian Federation, which has unity and consists of three ordered levels (subsystems):
· Subsystems of the federal level;
· Subsystems of the level of a constituent entity of the Russian Federation;
Subsystems of the level of the municipality
At the same time, at each level, the corresponding components of health care systems - state, municipal and private - should be legislatively enshrined and coordinated. To effectively solve such a problem, it is necessary in the NLA to concretize the ways to achieve the goals specified in the Constitution, establishing in particular: a) the organizational structure and competence of the managing component for the health care system at each level, not excluding the possibility of participation of representatives of the state, municipal and private health systems; b) the mandatory adoption of regulatory and individual acts of a higher-level control subsystem for its own level and lower-level subsystems should be ensured by the presence of specific measures of responsibility for non-compliance with these acts.
First of all, this should refer to federal legislation, which should be reflected and concretized in the legislation of the constituent entities of the Russian Federation and legal acts of local self-government bodies.
Along with this, it is necessary to abandon the accepted definition of health care as a system of public health management bodies and institutions subordinate to them, and to consolidate in the Federal Law a fundamentally new content of this concept as a system of relations aimed at protecting human health.
In many countries of the world, one of the main trends is the strengthening of the role of the state in the field of public health protection. The experience of delineating powers (decentralization) in the healthcare sector of foreign countries shows that, firstly, certain social and cultural conditions for decentralization are needed, which are gradually developing; second, decentralization has both positive and negative consequences; thirdly, in any case, some strategic areas remain outside the boundaries of decentralization, incl. principles of state policy in the sphere of salary, fourthly, there is no single optimal model that can be used without any special changes in the basis for the construction of federal relations in the sphere of salary.
The main problem at present is that the legislation regulating the health sector does not form the organizational unity of all parts of the system. As a result, the ongoing reforms, affecting the development of individual areas, do not ensure the consistency, dynamism and integrity of the reform process.
The success of reforms in health care is determined by a single scientifically grounded strategy containing ways to overcome the crisis in the entire social sphere. It is obvious that the modern social policy in health care, built on an objective knowledge of the factors forming a healthy population and the state of the country's economy, requires a detailed study of legal regulation in the industry.
For this, first of all, it is necessary to improve the legislation regulating legal relations in health care and ensuring the organizational unity of the system as a whole, as well as establishing the responsibility of the constituent entities of the Russian Federation at all levels for the state of health of the population. For the functioning of the unified health care system of the Russian Federation, it is necessary to develop a Federal Law on the coordination of health issues with the establishment of specific measures for its implementation, including administrative and criminal sanctions. The norms of this law should be concretized in the laws of the constituent entities of the Federation; in addition, both in the federal law and in the normative acts of the constituent entities of the Russian Federation, a boundary should be established for the exercise by municipalities of their powers.
Another important measure to ensure the organizational unity of health care, according to paragraph "p" of Art. 71 of the Constitution, the federal authorities should establish minimum sufficient social standards of medical care, provided with an adequate amount of funding. The need to establish minimum social standards is also provided for by the norm of paragraph 6 of Art. 4 of the Law "On General Principles of Organization of Local Self-Government in the Russian Federation" dated 28.8.1995, No. 154-FZ. In turn, the health care subsystems of the constituent entities of the Russian Federation must exercise regulatory impact on the municipal health care systems. The real way to establish the unity of the state health care system should be such a coordination of actions, which is based on the organizing influence of the federal system on the territorial and municipal systems.
The presence of legislative registration of the vertical of the healthcare management system, as well as meaningful interconnections of healthcare management bodies of the constituent entities of the Russian Federation, is the most important principle of healthcare management and gives the state healthcare system a complete pyramidal appearance with a developed lower level. For the state health care system, in our opinion, in any economic situation, administrative methods of management should be inherent, since these methods are fully consistent with the tasks that health authorities are called upon to solve: to ensure the implementation of a unified policy in the field of health care, coordinate the work of various services, control the quality of medical care, introduce standardization issues in medical activities, etc. At present, it is advisable to reduce the independence of medical organizations in the economic sphere, since they have freedom that is inadequate to their economic responsibility. One of the ways to legally restore the power influence of the federal health care system in the territory when creating an administrative vertical is, in our opinion, changing the relationship between the competence of state and municipal formations. It is important to establish in the Federal Law the grounds on which state and municipal health care institutions can be either allowed or denied the right to provide paid medical services. The problem here is the need to combine interests, both public and private; their balance, reflected in the law, must not only be measured economically, but also give this regulation. In our opinion, the commercial activity of state and municipal healthcare organizations is an undesirable phenomenon for two reasons. First, the power represented by the committees will suppress the medical services market in every possible way. Secondly, the government will be corrupted. This means that it is necessary to introduce this power into a framework: on the one hand, to give it the opportunity to protect the public interest, on the other, not to give the opportunity to infringe on the private health care system. The owner of the municipal health care organizations is the population of the territories, and only it is necessary to be guided by it when solving all issues. The health care system, as well as other sectors of the social sphere, faces the problem of privatization associated with the optimal construction of the system of organization and management. And here, it seems to me, we must take into account one incongruity that has arisen in our law. We have essentially abandoned the variety of forms of ownership. We know only state, municipal and private, it is not clear why we have discarded collective property, But you cannot transfer most of the medical complexes into private hands. Even if there is such a structure that will swallow all this, such an option is undesirable from the point of view of the interests of the population. Therefore, it is advisable to revive collective property. And yet, according to the current legislation, it is possible to approach the privatization of one or another healthcare organization as an object without taking into account the processes in which this object is involved. We propose that during privatization we consider not objects, but completely different entities, consisting of peculiar processes. When preparing a healthcare organization for privatization, it is necessary to consider its activities in a complex and to determine in two aspects:
1. Subject of privatization - all infrastructural processes remain in state (municipal) ownership;
2. All fast processes are moving into the private health care system.
Conclusion
It is necessary to take for granted the fact that in the transition period one cannot do without a rigid regulatory function of the state and law in building a new health care system. To rush into the market (create a multi-structure) without a legal basis means to reproduce the conditions of the period of initial capital accumulation with all the ensuing socio-political consequences that our country went through in 1992-1995. Law not only reflects the existing social system, but also acts as a regulator of social relations, bringing the behavior of people and organizations in line with the interests of society. The law plays a leading role in defining the principles of the activities of organizations and the activities of state health authorities, their competence, the form and procedure for solving new problems by them.
Having analyzed the situation in healthcare, we propose the following set of measures to improve the availability and quality of medical care.
1) Having decided to support primary health care at the federal level, the regions should be much more active in supporting primary health care. There is understanding and striving for this in the regions. But we need a mechanism that will allow directing funds from regional budgets directly to municipal medical institutions, bypassing municipalities, for example, through regional health authorities. Otherwise, the municipality will be tempted to spend money on other, equally important and urgent needs.
2) To increase the availability of high-tech medical care, it is advisable to combine the centers of high medical technologies into single all-Russian specialized medical services with branches in the regions. This will ensure the development of unified standards for diagnostics, treatment, medical rehabilitation, a unified methodology for training highly qualified medical personnel. It will increase the coordinating role of the Ministry of Health and Social Development of Russia, which is especially important in these conditions of the redistribution of powers and the transfer to regional and municipal levels of a significant part of the obligations to provide medical care to the population.
3) Prevention should take a special place. At all levels, target programs for the prevention of diseases should be developed already this year, including programs for general medical examination, vaccination of the population, especially, of course, children.
Along with this, it is extremely necessary to establish a widespread healthy lifestyle, the formation of a kind of cult of health, the development of physical culture and sports. This also requires special programs at all levels.
4) With regard to the material and technical base, the most urgent, namely, the equipment of the primary care has already been provided. But the decline in the domestic production of medical equipment, modern complex medical equipment and medicines is obvious.
Therefore, it is necessary to develop and implement federal targeted programs for the development of the medical and pharmaceutical industry in Russia.
5) The key link in the system of measures to improve the accessibility and quality of medical care should be strengthening the human resources of health care and a radical improvement in the social well-being of medical workers. Make the amount of remuneration in health care dependent on the quality of medical services, and introduce a number of organizational measures to increase responsibility for the improper provision of medical services.
In addition, along with the support of primary care staff, we are obliged to provide measures to retain specialists of the highest category.
6) No systemic changes in health care will go without improving its legislative base. The basic, system-forming law on healthcare in the Russian Federation has not yet been adopted.
The main directions in improving the organization of medical care are the development of primary health care on the basis of municipal health care, the redistribution of part of the volume of care from the inpatient sector to the outpatient one.
Primary health care is the main link in the provision of medical care to the population.
A special role is given to the development of the institution of general (family) practice. Consultative and diagnostic services should be developed in polyclinics. On their basis, departments of medical and social rehabilitation and therapy, nursing services, day hospitals, centers for outpatient surgery and medical and social assistance, etc. can be deployed.
Measures to introduce modern technologies in intensive care units, cardiology and cardiac surgery, oncology, diagnostics and treatment of socially significant diseases require state support.
It is necessary to strengthen the ambulance service, make it more mobile and equipped with modern facilities for the provision of emergency medical care and emergency hospitalization of patients.
It is required to increase the role of scientific centers and research institutes in the development and implementation of effective medical technologies, the use of unique methods of diagnosis and treatment.
It is necessary to take measures of state support to improve rehabilitation assistance, the development of sanatorium-resort organizations of the health care system, health institutions and organizations.
To improve the quality and accessibility of medical care to the rural population, it is necessary to form medical and diagnostic complexes on the basis of central regional hospitals, including municipal rural medical institutions, to develop mobile forms of medical diagnostic and advisory assistance, to create interdistrict clinical diagnostic centers.
It is necessary to integrate departmental medical institutions into the general health care system on a single regulatory and legal basis, taking into account their industry characteristics and location.
The emerging private sector will play an important role while maintaining the dominant role of public and municipal health care.
The creation of conditions for its development is an essential element of structural transformations in health care.
It is necessary to ensure that medical organizations, individuals engaged in private medical activities, state and municipal organizations have equal rights to work in the compulsory health insurance system and to participate in the implementation of state and municipal targeted programs. The participation of medical organizations of various forms of ownership in the implementation of state health programs, municipal orders should be carried out on a competitive basis.
State and municipal medical institutions performing functions that are not bound by the framework of a unified technology for the provision of medical care should have broad powers in matters of property use and staff remuneration.
Bibliography
1. The Constitution of the Russian Federation: Adopted by popular vote on December 12, 1993 (as amended on July 25, 2003) // SZ RF.-2003.
2. Decree of the Government of the Russian Federation of November 5, 1997 No. 1387 "On measures to stabilize and develop health care and medical science in the Russian Federation."
3. The concept of development of health care and medical science in the Russian Federation. M., 2005.
4. Fundamentals of the legislation of the Russian Federation on the protection of the health of citizens of 07.03.2005.
5. Belova N.V., Suslonova N.V. Preservation of health care // Problems of health care management. 2004. No. 1 (14). S. 7-8.
6. Galkin R.A. Sandreeva S.Kh., Fedoseeva L.S. Healthcare // Problems of healthcare management. 2001. No. 2. S. 38-40.
7. Galkin R.A., Gekht I.A. Suslin S.A. Organization of medical and social assistance to the elderly in rural areas. Samara, 2001 .-- 512 p.
8. Kalininskaya A.A. Gudanova E.N., Matveev E.N. Health economics // Problems of social hygiene, health care and history of medicine. 2002. No. 1. S. 43-46.
9. Kirillov A.V. Health problems // Russian family doctor. 2001. No. 1. S. 43.
10. Kozhevnikov V.V. Problems of Territorial Health Care: Collection of Scientific Papers. M., 2003. Issue. 5. - 112 p.
11. Lakunin K.Yu. Provision of medical care for the population of rural municipalities and approaches to planning it in the new socio-economic conditions: Abstract dis. ... Dr. med. Science. M., 2001.
12. Ludyapova E.Yu. Organizational and economic substantiation of the use of hospital-replacing technologies in rural areas: Abstract dis. ... Cand. Honey. Science. SPb, 2002.S. 40.
13. Mikhailova Yu.V., Magnitsky V.A. Healthcare // Chief physician. 2004. No. 9.P. 30.
14. Mikhailova Yu.V., Magnitsky V.A. Health care management // Chief physician. 2002. No. 6. P. 4.
15. Public health and health care. Textbook Public health and health care. Textbook for universities / Ed. Yu. P. Lisitsyna. M .: UNITI-DANA, 2006 .-- 668 p.
16. Pascal A.V. Scientific substantiation of organizational forms and ways to improve the efficiency and quality of out-of-hospital care for the rural population of the region (on the example of the Saratov region): Abstract dis. ... Cand. Honey. Science. SPb, 2002.S. 44.
17. Petrov P.P., Kalzhekov T.K. Problems of organizing medical care for the rural population. Alma-Ata, 1990 .-- 328 p.
18. Semenov V.Yu., Tamazyan G.V., Mikhnevich N.N. and other Management in the field of health // Health. 2004. No. 5.P. 32.
19. Stepanov V.V., Finchenko E.A. The main directions of rural health care. Novosibirsk, 2003 .-- 228 p.
20. Tatarnikov M.A. Health care reform in the Russian Federation: problems and prospects for their solution. M .: UNITI-DANA, 2003 .-- 336 p.
21. Finchenko E.A., Stepanov V.V. Healthcare // Problems of healthcare management. 2003. No. 5 (12). S. 5-13.
22. Shchipin V.O. Structural transformation in health care. M .: Unity, 1997 .-- 448 p.
Mikhailova Yu.V., Magnitsky V.A. Health care management // Chief physician. 2002. No. 6. P. 4.
Public health and healthcare. Textbook Public health and health care. Textbook for universities / Ed. Yu. P. Lisitsyna. M .: UNITI-DANA, 2006.S. 81.
Public health and healthcare. Textbook Public health and health care. Textbook for universities / Ed. Yu. P. Lisitsyna. M .: UNITI-DANA, 2006.S. 90-91.
Public health and healthcare. Textbook Public health and health care. Textbook for universities / Ed. Yu. P. Lisitsyna. M .: UNITI-DANA, 2006.S. 99.
Public health and healthcare. Textbook Public health and health care. Textbook for universities / Ed. Yu. P. Lisitsyna. M .: UNITI-DANA, 2006.S. 103.
Public health and healthcare. Textbook Public health and health care. Textbook for universities / Ed. Yu. P. Lisitsyna. M .: UNITI-DANA, 2006.S. 105.
Lakunin K.Yu. Provision of medical care for the population of rural municipalities and approaches to planning it in the new socio-economic conditions: Abstract dis. ... Dr. med. Science. M., 2001.
Kalininskaya A.A. Gudanova E.N., Matveev E.N. Health economics // Problems of social hygiene, health care and history of medicine. 2002. No. 1. S. 43-46.
Shchipin V.O. Structural transformation in health care. M .: Unity, 1997.S. 113.
Stepanov V.V., Finchenko E.A. The main directions of rural health care. Novosibirsk, 2003.S. 106.
Petrov P.P., Kalzhekov T.K. Problems of organizing medical care for the rural population. Alma-Ata, 1990.S. 200.
Pascal A.V. Scientific substantiation of organizational forms and ways to improve the efficiency and quality of out-of-hospital care for the rural population of the region (on the example of the Saratov region): Abstract dis. ... Cand. Honey. Science. SPb, 2002.S. 44.
Ludyapova E.Yu. Organizational and economic substantiation of the use of hospital-replacing technologies in rural areas: Abstract dis. ... Cand. Honey. Science. SPb, 2002.S. 40.
V.V. Kozhevnikov Problems of Territorial Health Care: Collection of Scientific Papers. M., 2003. Issue. 5.S. 66-70.
Galkin R.A., Gekht I.A. Suslin S.A. Organization of medical and social assistance to elderly people in rural areas. Samara, 2001.S. 30.
See: Yu.V. Mikhailova, V.A. Magnitsky. Healthcare // Chief physician. 2004. No. 9.P. 30.
Public health and healthcare. Textbook Public health and health care. Textbook for universities / Ed. Yu. P. Lisitsyna. M .: UNITI-DANA, 2006.S. 107.
Related Articles